

Immune-based classification of HPV-associated oropharyngeal cancer with implications for biomarker-driven treatment de-intensification
- PMID: 36442320
- PMCID: PMC9706534
- DOI: 10.1016/j.ebiom.2022.104373
Immune-based classification of HPV-associated oropharyngeal cancer with implications for biomarker-driven treatment de-intensification
Abstract
Background: There is significant interest in treatment de-escalation for human papillomavirus-associated (HPV+) oropharyngeal squamous cell carcinoma (OPSCC) patients given the generally favourable prognosis. However, 15-30% of patients recur after primary treatment, reflecting a need for improved risk-stratification tools. We sought to develop a molecular test to risk stratify HPV+ OPSCC patients.
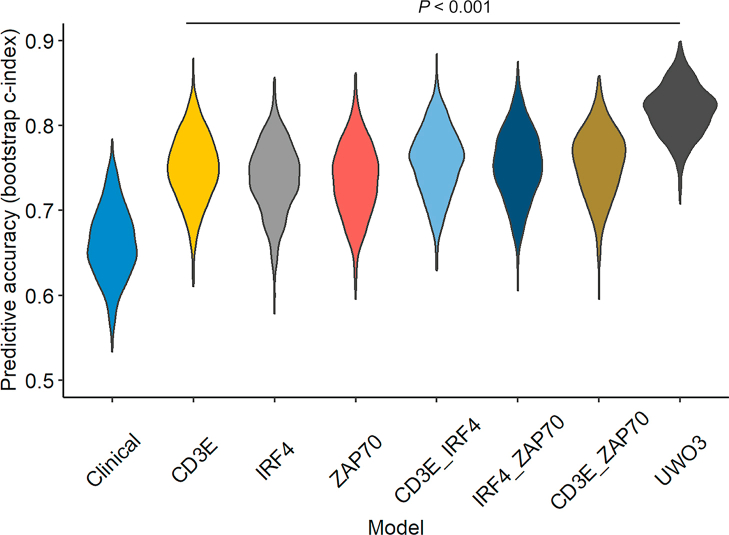
Methods: We created an immune score (UWO3) associated with survival outcomes in six independent cohorts comprising 906 patients, including blinded retrospective and prospective external validations. Two aggressive radiation de-escalation cohorts were used to assess the ability of UWO3 to identify patients who recur. Multivariate Cox models were used to assess the associations between the UWO3 immune class and outcomes.
Findings: A three-gene immune score classified patients into three immune classes (immune rich, mixed, or immune desert) and was strongly associated with disease-free survival in six datasets, including large retrospective and prospective datasets. Pooled analysis demonstrated that the immune rich group had superior disease-free survival compared to the immune desert (HR = 9.0, 95% CI: 3.2-25.5, P = 3.6 × 10-5) and mixed (HR = 6.4, 95% CI: 2.2-18.7, P = 0.006) groups after adjusting for age, sex, smoking status, and AJCC8 clinical stage. Finally, UWO3 was able to identify patients from two small treatment de-escalation cohorts who remain disease-free after aggressive de-escalation to 30 Gy radiation.
Interpretation: With additional prospective validation, the UWO3 score could enable biomarker-driven clinical decision-making for patients with HPV+ OPSCC based on robust outcome prediction across six independent cohorts. Prospective de-escalation and intensification clinical trials are currently being planned.
Funding: CIHR, European Union, and the NIH.
Keywords: Biomarkers; Cancer immunology; De-escalation; HPV; Head and neck squamous cell carcinoma; Transcriptomics.
Copyright © 2022 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests PYFZ, JWB, PCB, JSM and ACN have a US patent pending for the UWO3 score. All other authors declare no conflict of interest.
Figures










References
-
- Menezes F.D.S., Fernandes G.A., Antunes J.L.F., Villa L.L., Toporcov T.N. Global incidence trends in head and neck cancer for HPV-related and -unrelated subsites: a systematic review of population-based studies. Oral Oncol. 2021;115 - PubMed
-
- Cramer J.D., Burtness B., Le Q.T., Ferris R.L. The changing therapeutic landscape of head and neck cancer. Nat Rev Clin Oncol. 2019;16:669–683. - PubMed
-
- Nichols A.C., Finkelstein D.M., Faquin W.C., et al. Bcl2 and human papilloma virus 16 as predictors of outcome following concurrent chemoradiation for advanced oropharyngeal cancer. Clin Cancer Res. 2010;16(7):2138–2146. - PubMed
