

Pregnancy outcomes after first-trimester treatment with artemisinin derivatives versus non-artemisinin antimalarials: a systematic review and individual patient data meta-analysis
- PMID: 36442488
- PMCID: PMC9874756
- DOI: 10.1016/S0140-6736(22)01881-5
Pregnancy outcomes after first-trimester treatment with artemisinin derivatives versus non-artemisinin antimalarials: a systematic review and individual patient data meta-analysis
Abstract
Background: Malaria in the first trimester of pregnancy is associated with adverse pregnancy outcomes. Artemisinin-based combination therapies (ACTs) are a highly effective, first-line treatment for uncomplicated Plasmodium falciparum malaria, except in the first trimester of pregnancy, when quinine with clindamycin is recommended due to concerns about the potential embryotoxicity of artemisinins. We compared adverse pregnancy outcomes after artemisinin-based treatment (ABT) versus non-ABTs in the first trimester of pregnancy.
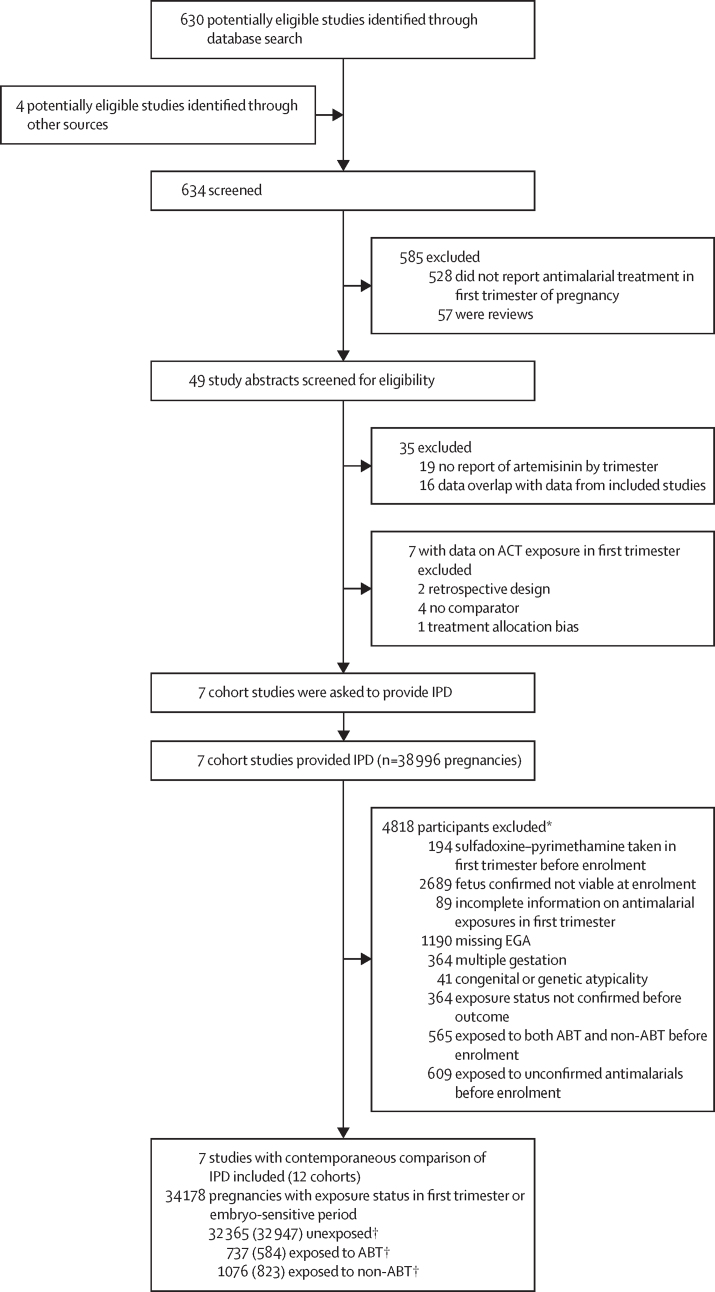
Methods: For this systematic review and individual patient data (IPD) meta-analysis, we searched MEDLINE, Embase, and the Malaria in Pregnancy Library for prospective cohort studies published between Nov 1, 2015, and Dec 21, 2021, containing data on outcomes of pregnancies exposed to ABT and non-ABT in the first trimester. The results of this search were added to those of a previous systematic review that included publications published up until November, 2015. We included pregnancies enrolled before the pregnancy outcome was known. We excluded pregnancies with missing estimated gestational age or exposure information, multiple gestation pregnancies, and if the fetus was confirmed to be unviable before antimalarial treatment. The primary endpoint was adverse pregnancy outcome, defined as a composite of either miscarriage, stillbirth, or major congenital anomalies. A one-stage IPD meta-analysis was done by use of shared-frailty Cox models. This study is registered with PROSPERO, number CRD42015032371.
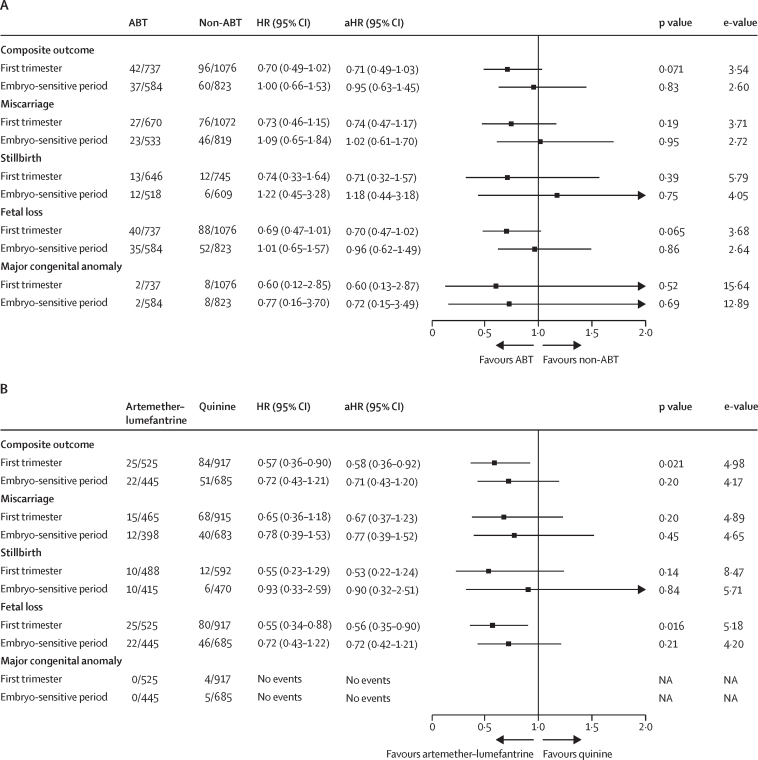
Findings: We identified seven eligible studies that included 12 cohorts. All 12 cohorts contributed IPD, including 34 178 pregnancies, 737 with confirmed first-trimester exposure to ABTs and 1076 with confirmed first-trimester exposure to non-ABTs. Adverse pregnancy outcomes occurred in 42 (5·7%) of 736 ABT-exposed pregnancies compared with 96 (8·9%) of 1074 non-ABT-exposed pregnancies in the first trimester (adjusted hazard ratio [aHR] 0·71, 95% CI 0·49-1·03). Similar results were seen for the individual components of miscarriage (aHR=0·74, 0·47-1·17), stillbirth (aHR=0·71, 0·32-1·57), and major congenital anomalies (aHR=0·60, 0·13-2·87). The risk of adverse pregnancy outcomes was lower with artemether-lumefantrine than with oral quinine in the first trimester of pregnancy (25 [4·8%] of 524 vs 84 [9·2%] of 915; aHR 0·58, 0·36-0·92).
Interpretation: We found no evidence of embryotoxicity or teratogenicity based on the risk of miscarriage, stillbirth, or major congenital anomalies associated with ABT during the first trimester of pregnancy. Given that treatment with artemether-lumefantrine was associated with fewer adverse pregnancy outcomes than quinine, and because of the known superior tolerability and antimalarial effectiveness of ACTs, artemether-lumefantrine should be considered the preferred treatment for uncomplicated P falciparum malaria in the first trimester. If artemether-lumefantrine is unavailable, other ACTs (except artesunate-sulfadoxine-pyrimethamine) should be preferred to quinine. Continued active pharmacovigilance is warranted.
Funding: Medicines for Malaria Venture, WHO, and the Worldwide Antimalarial Resistance Network funded by the Bill & Melinda Gates Foundation.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
First-trimester use of ACTs for malaria treatment in pregnancy.Lancet. 2023 Jan 14;401(10371):81-83. doi: 10.1016/S0140-6736(22)02166-3. Epub 2022 Nov 25. Lancet. 2023. PMID: 36442486 No abstract available.
References
-
- Moeller SL, Nyengaard JR, Larsen LG, et al. Malaria in early pregnancy and the development of the placental vasculature. J Infect Dis. 2019;220:1425–1434. - PubMed
-
- Schmiegelow C, Matondo S, Minja DTR, et al. Plasmodium falciparum infection early in pregnancy has profound consequences for fetal growth. J Infect Dis. 2017;216:1601–1610. - PubMed
-
- Huynh BT, Cottrell G, Cot M, Briand V. Burden of malaria in early pregnancy: a neglected problem? Clin Infect Dis. 2015;60:598–604. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
