

Harmonizing Definitions for Diagnostic Criteria and Prognostic Assessment of Transplantation-Associated Thrombotic Microangiopathy: A Report on Behalf of the European Society for Blood and Marrow Transplantation, American Society for Transplantation and Cellular Therapy, Asia-Pacific Blood and Marrow Transplantation Group, and Center for International Blood and Marrow Transplant Research
- PMID: 36442770
- PMCID: PMC10119629
- DOI: 10.1016/j.jtct.2022.11.015
Harmonizing Definitions for Diagnostic Criteria and Prognostic Assessment of Transplantation-Associated Thrombotic Microangiopathy: A Report on Behalf of the European Society for Blood and Marrow Transplantation, American Society for Transplantation and Cellular Therapy, Asia-Pacific Blood and Marrow Transplantation Group, and Center for International Blood and Marrow Transplant Research
Abstract
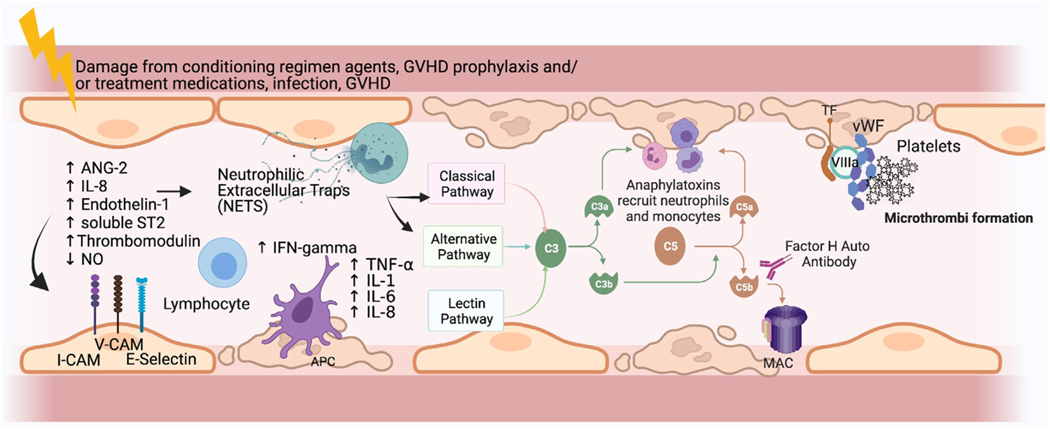
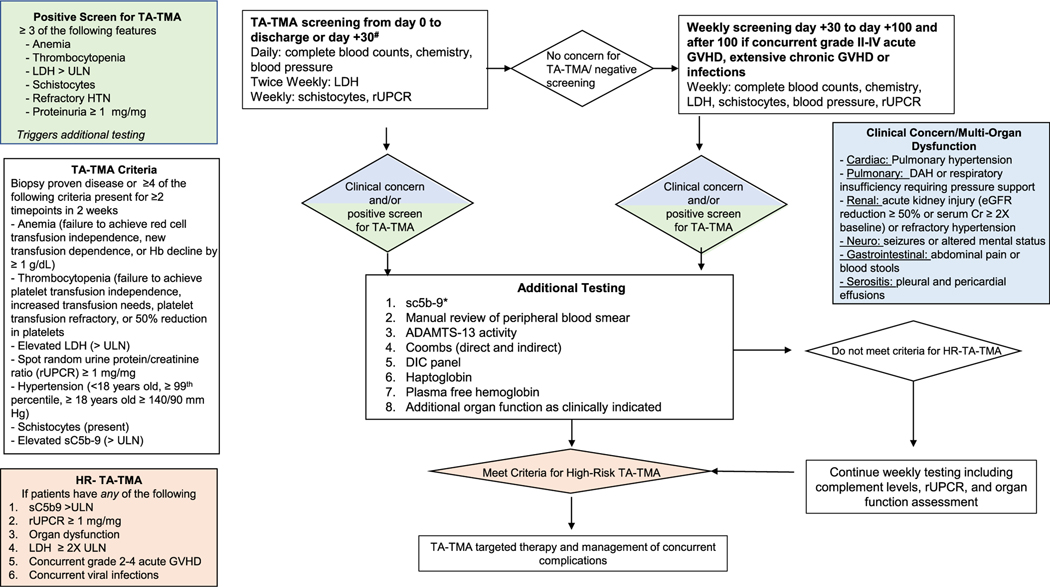
Transplantation-associated thrombotic microangiopathy (TA-TMA) is an increasingly recognized complication of hematopoietic cell transplantation (HCT) associated with significant morbidity and mortality. However, TA-TMA is a clinical diagnosis, and multiple criteria have been proposed without universal application. Although some patients have a self-resolving disease, others progress to multiorgan failure and/or death. Poor prognostic features also are not uniformly accepted. The lack of harmonization of diagnostic and prognostic markers has precluded multi-institutional studies to better understand incidence and outcomes. Even current interventional trials use different criteria, making it challenging to interpret the data. To address this urgent need, the American Society for Transplantation and Cellular Therapy, Center for International Bone Marrow Transplant Research, Asia-Pacific Blood and Marrow Transplantation, and European Society for Blood and Marrow Transplantation nominated representatives for an expert panel tasked with reaching consensus on diagnostic and prognostic criteria. The panel reviewed literature, generated consensus statements regarding diagnostic and prognostic features of TA-TMA using the Delphi method, and identified future directions of investigation. Consensus was reached on 4 key concepts: (1) TA-TMA can be diagnosed using clinical and laboratory criteria or tissue biopsy of kidney or gastrointestinal tissue; however, biopsy is not required; (2) consensus diagnostic criteria are proposed using the modified Jodele criteria with additional definitions of anemia and thrombocytopenia. TA-TMA is diagnosed when ≥4 of the following 7 features occur twice within 14 days: anemia, defined as failure to achieve transfusion independence despite neutrophil engraftment; hemoglobin decline by ≥1 g/dL or new-onset transfusion dependence; thrombocytopenia, defined as failure to achieve platelet engraftment, higher-than-expected transfusion needs, refractory to platelet transfusions, or ≥50% reduction in baseline platelet count after full platelet engraftment; lactate dehydrogenase (LDH) exceeding the upper limit of normal (ULN); schistocytes; hypertension; soluble C5b-9 (sC5b-9) exceeding the ULN; and proteinuria (≥1 mg/mg random urine protein-to-creatinine ratio [rUPCR]); (3) patients with any of the following features are at increased risk of nonrelapse mortality and should be stratified as high-risk TA-TMA: elevated sC5b-9, LDH ≥2 times the ULN, rUPCR ≥1 mg/mg, multiorgan dysfunction, concurrent grade II-IV acute graft-versus-host disease (GVHD), or infection (bacterial or viral); and (4) all allogeneic and pediatric autologous HCT recipients with neuroblastoma should be screened weekly for TA-TMA during the first 100 days post-HCT. Patients diagnosed with TA-TMA should be risk-stratified, and those with high-risk disease should be offered participation in a clinical trial for TA-TMA-directed therapy if available. We propose that these criteria and risk stratification features be used in data registries, prospective studies, and clinical practice across international settings. This harmonization will facilitate the investigation of TA-TMA across populations diverse in race, ethnicity, age, disease indications, and transplantation characteristics. As these criteria are widely used, we expect continued refinement as necessary. Efforts to identify more specific diagnostic and prognostic biomarkers are a top priority of the field. Finally, an investigation of the impact of TA-TMA-directed treatment, particularly in the setting of concurrent highly morbid complications, such as steroid-refractory GVHD and infection, is critically needed.
Keywords: Complement; Diagnostic criteria; Nonrelapse mortality; Risk stratification; Transplantation-associated thrombotic microangiopathy.
Copyright © 2022 The American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest statement:
B.E.S. reports consulting for Mallinckrodt and Orca Bio; C.E.D. reports consulting for Omeros and Alexion; S.V. reports serving on an advisory board for Omeros; S. J. is named on US Patent 10,815,296 B2 as a principal investigator for a drug provided by Alexion and consulting for and honoraria from Omeros, SOBI, Alexion, and MedScape; and V.H. reports consulting for Alexion and Omeros and research funding from CareDx, Jazz Pharmaceuticals, and Omeros.
Figures
References
-
- Gavriilaki E, Touloumenidou T, Sakellari I, et al. Pretransplant genetic susceptibility: clinical relevance in transplant-associated thrombotic microangiopathy. Thromb Haemost. 2020;120:638–646. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
