

mTORC1 links pathology in experimental models of Still's disease and macrophage activation syndrome
- PMID: 36443301
- PMCID: PMC9705324
- DOI: 10.1038/s41467-022-34480-6
mTORC1 links pathology in experimental models of Still's disease and macrophage activation syndrome
Abstract
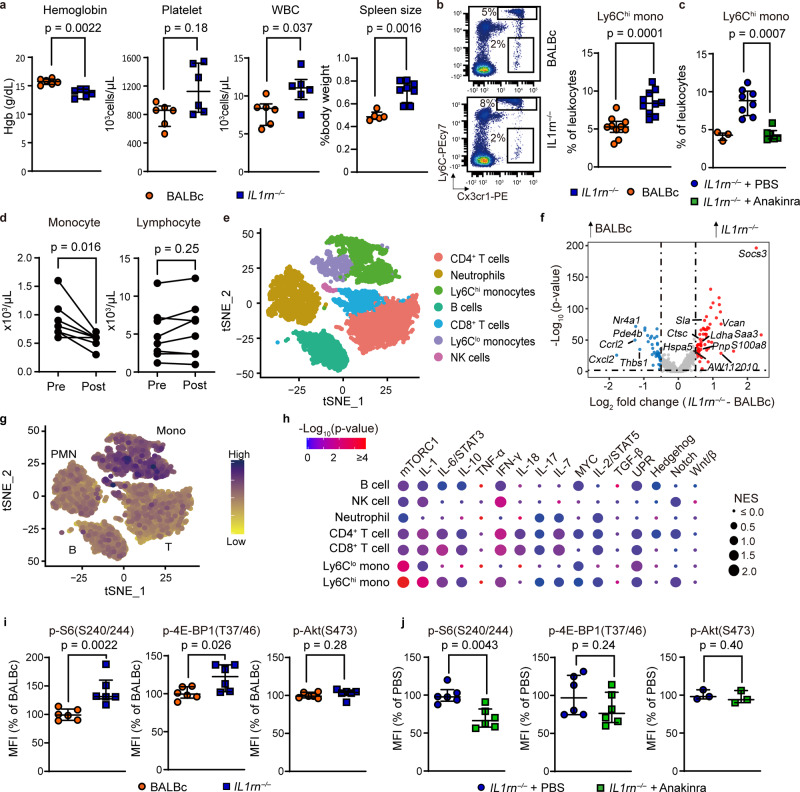
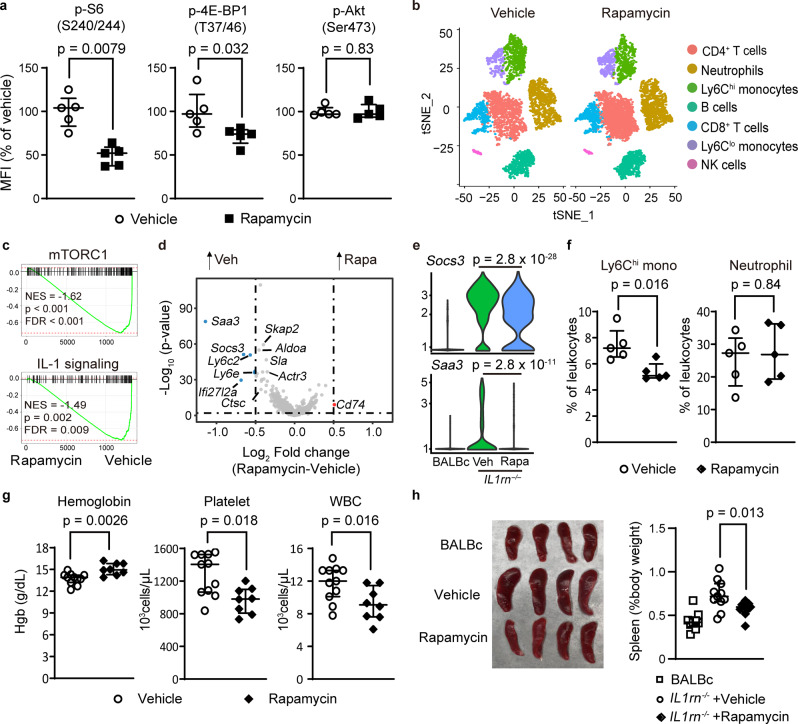
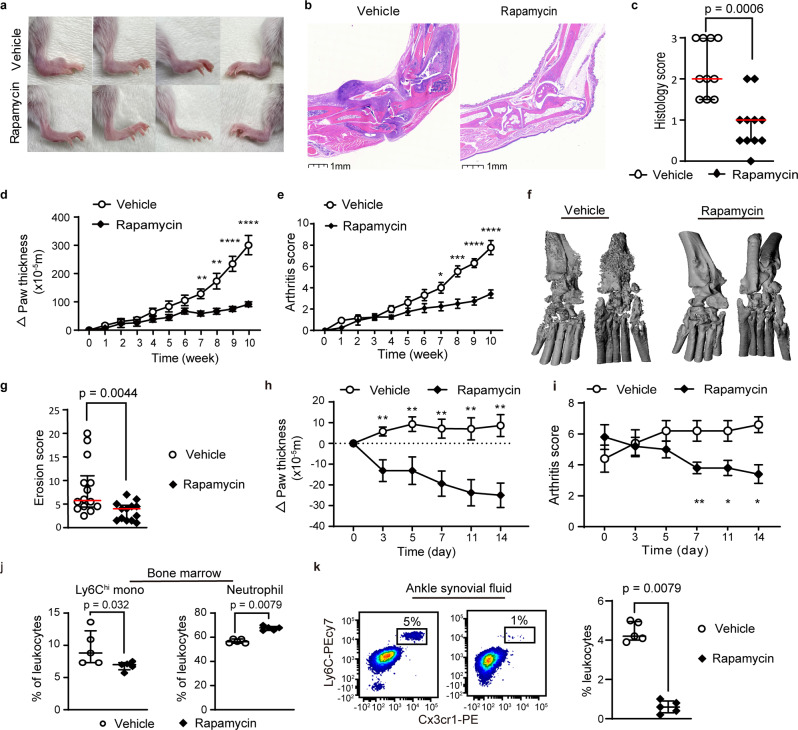
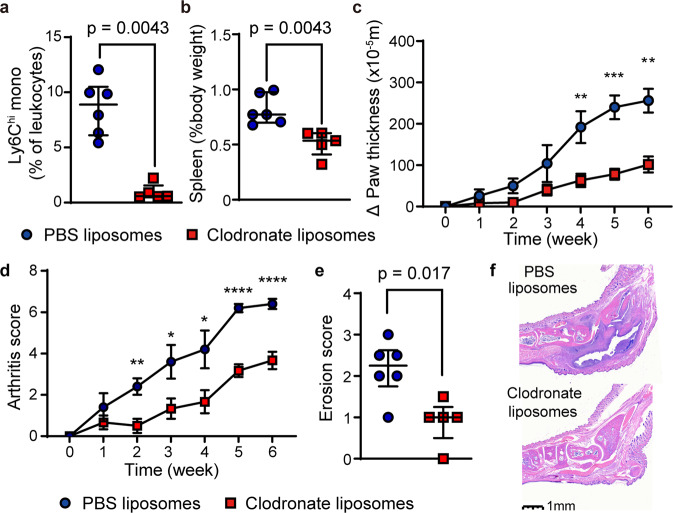
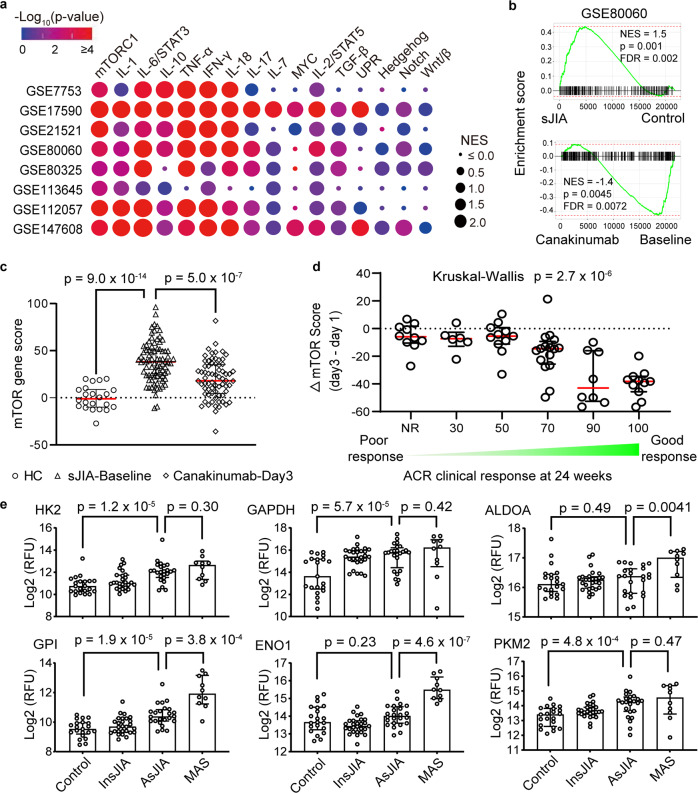
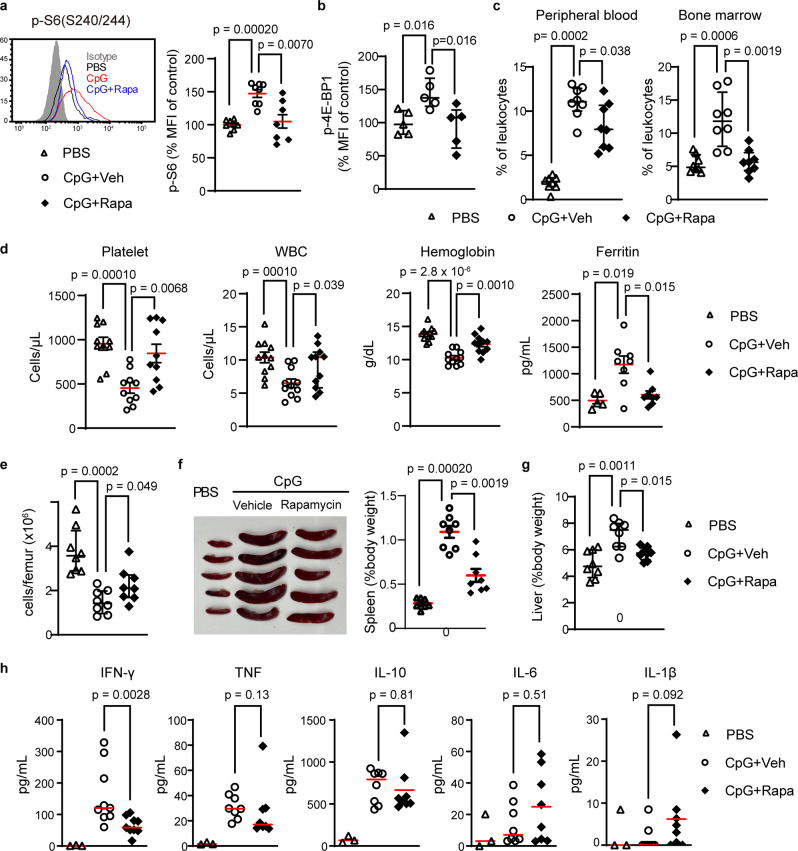
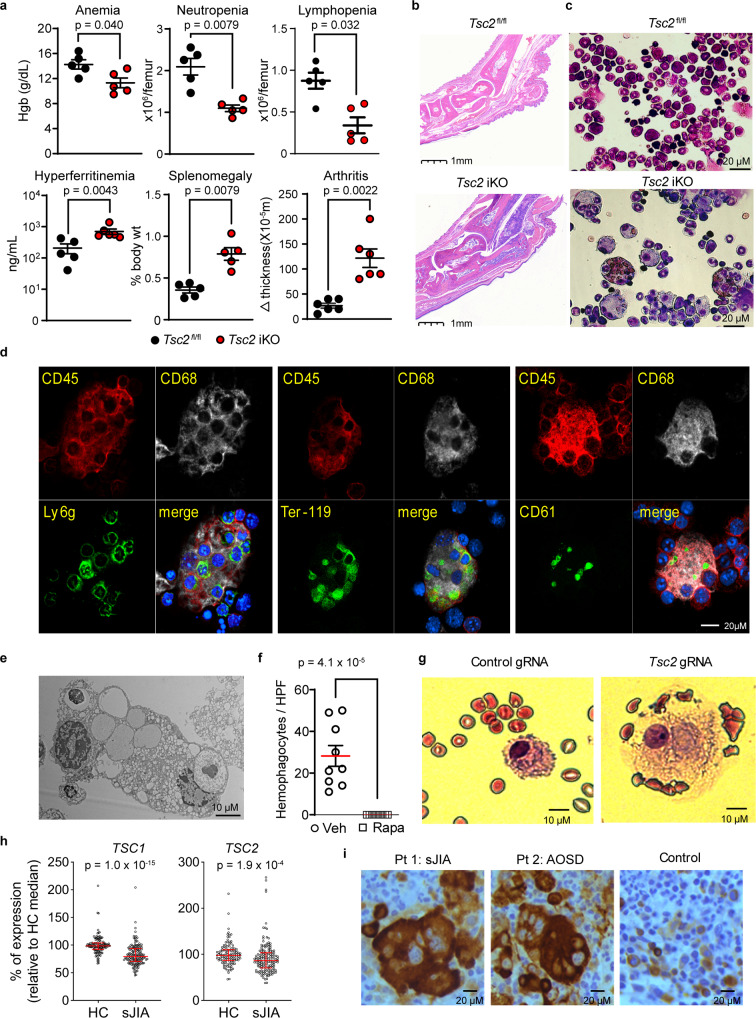
Still's disease is a severe inflammatory syndrome characterized by fever, skin rash and arthritis affecting children and adults. Patients with Still's disease may also develop macrophage activation syndrome, a potentially fatal complication of immune dysregulation resulting in cytokine storm. Here we show that mTORC1 (mechanistic target of rapamycin complex 1) underpins the pathology of Still's disease and macrophage activation syndrome. Single-cell RNA sequencing in a murine model of Still's disease shows preferential activation of mTORC1 in monocytes; both mTOR inhibition and monocyte depletion attenuate disease severity. Transcriptomic data from patients with Still's disease suggest decreased expression of the mTORC1 inhibitors TSC1/TSC2 and an mTORC1 gene signature that strongly correlates with disease activity and treatment response. Unrestricted activation of mTORC1 by Tsc2 deletion in mice is sufficient to trigger a Still's disease-like syndrome, including both inflammatory arthritis and macrophage activation syndrome with hemophagocytosis, a cellular manifestation that is reproduced in human monocytes by CRISPR/Cas-mediated deletion of TSC2. Consistent with this observation, hemophagocytic histiocytes from patients with macrophage activation syndrome display prominent mTORC1 activity. Our study suggests a mechanistic link of mTORC1 to inflammation that connects the pathogenesis of Still's disease and macrophage activation syndrome.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
mTORC1 implicated in Still's disease and MAS.Nat Rev Rheumatol. 2023 Feb;19(2):64. doi: 10.1038/s41584-023-00908-6. Nat Rev Rheumatol. 2023. PMID: 36609688 No abstract available.
References
-
- Davies R, et al. Mortality rates are increased in patients with systemic juvenile idiopathic arthritis. Arch. Dis. Child. 2017;102:206–207. - PubMed
-
- Minoia F, et al. Clinical features, treatment, and outcome of macrophage activation syndrome complicating systemic juvenile idiopathic arthritis: a multinational, multicenter study of 362 patients. Arthritis Rheumatol. 2014;66:3160–3169. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
