

Safety and efficacy of human polymerized hemoglobin on guinea pig resuscitation from hemorrhagic shock
- PMID: 36443351
- PMCID: PMC9703428
- DOI: 10.1038/s41598-022-23926-y
Safety and efficacy of human polymerized hemoglobin on guinea pig resuscitation from hemorrhagic shock
Abstract
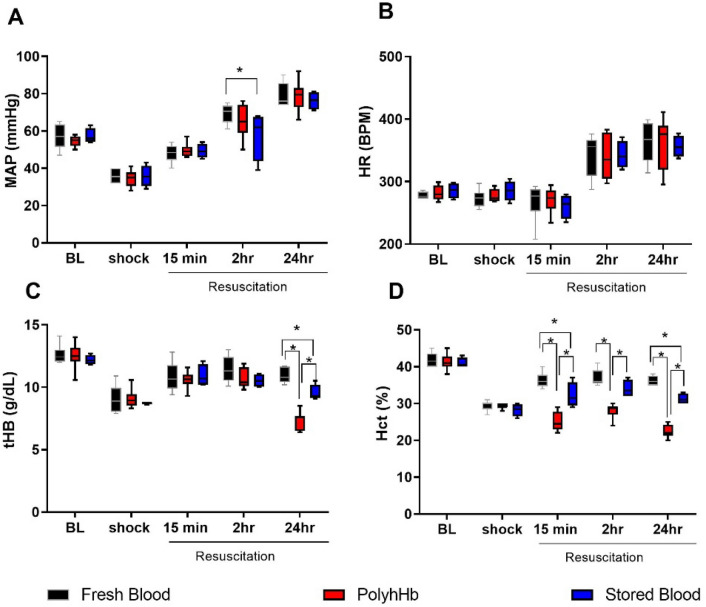
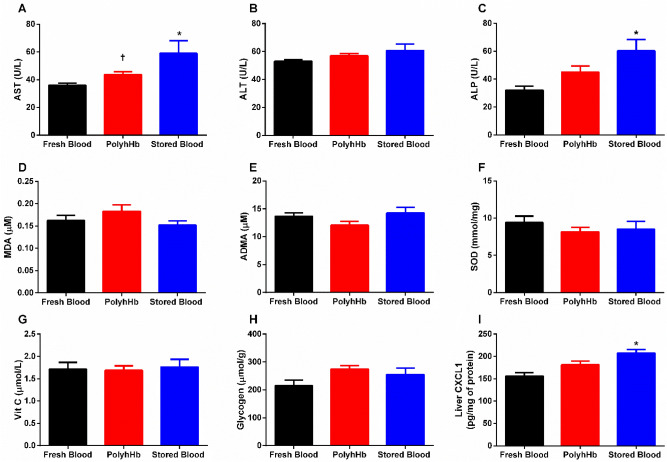
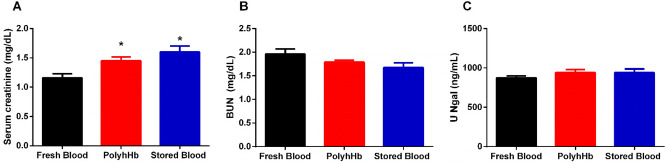
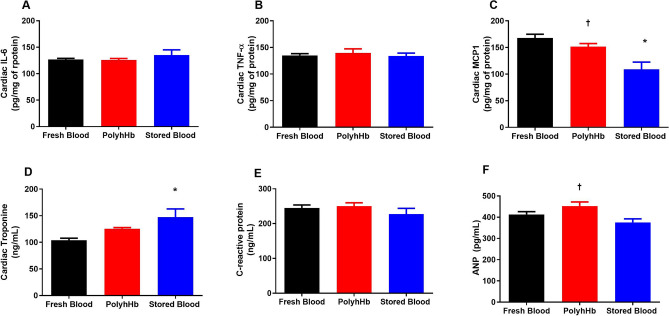
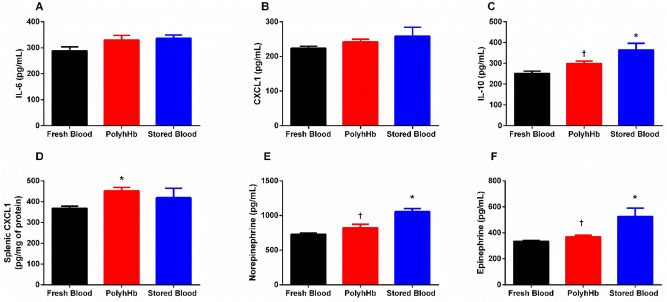
For the past thirty years, hemoglobin-based oxygen carriers (HBOCs) have been under development as a red blood cell substitute. Side-effects such as vasoconstriction, oxidative injury, and cardiac toxicity have prevented clinical approval of HBOCs. Recently, high molecular weight (MW) polymerized human hemoglobin (PolyhHb) has shown positive results in rats. Studies have demonstrated that high MW PolyhHb increased O2 delivery, with minimal effects on blood pressure, without vasoconstriction, and devoid of toxicity. In this study, we used guinea pigs to evaluate the efficacy and safety of high MW PolyhHb, since like humans guinea pigs cannot produce endogenous ascorbic acid, which limits the capacity of both species to deal with oxidative stress. Hence, this study evaluated the efficacy and safety of resuscitation from severe hemorrhagic shock with high MW PolyhHb, fresh blood, and blood stored for 2 weeks. Animals were randomly assigned to each experimental group, and hemorrhage was induced by the withdrawal of 40% of the blood volume (BV, estimated as 7.5% of body weight) from the carotid artery catheter. Hypovolemic shock was maintained for 50 min. Resuscitation was implemented by infusing 25% of the animal's BV with the different treatments. Hemodynamics, blood gases, total hemoglobin, and lactate were not different before hemorrhage and during shock between groups. The hematocrit was lower for the PolyhHb group compared to the fresh and stored blood groups after resuscitation. Resuscitation with stored blood had lower blood pressure compared to fresh blood at 2 h. There was no difference in mean arterial pressure between groups at 24 h. Resuscitation with PolyhHb was not different from fresh blood for most parameters. Resuscitation with PolyhHb did not show any remarkable change in liver injury, inflammation, or cardiac damage. Resuscitation with stored blood showed changes in liver function and inflammation, but no kidney injury or systemic inflammation. Resuscitation with stored blood after 24 h displayed sympathetic hyper-activation and signs of cardiac injury. These results suggest that PolyhHb is an effective resuscitation alternative to blood. The decreased toxicities in terms of cardiac injury markers, vital organ function, and inflammation following PolyhHb resuscitation in guinea pigs indicate a favorable safety profile. These results are promising and support future studies with this new generation of PolyhHb as alternative to blood when blood is unavailable.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Polymerized human hemoglobin with low and high oxygen affinity in trauma models.Transl Res. 2023 Oct;260:83-92. doi: 10.1016/j.trsl.2023.05.006. Epub 2023 Jun 1. Transl Res. 2023. PMID: 37268039
-
The Molecular Size of Bioengineered Oxygen Carriers Determines Tissue Oxygenation in a Hypercholesterolemia Guinea Pig Model of Hemorrhagic Shock and Resuscitation.Mol Pharm. 2023 Nov 6;20(11):5739-5752. doi: 10.1021/acs.molpharmaceut.3c00611. Epub 2023 Oct 16. Mol Pharm. 2023. PMID: 37843033
-
Resuscitation from hemorrhagic shock after traumatic brain injury with polymerized hemoglobin.Sci Rep. 2021 Jan 28;11(1):2509. doi: 10.1038/s41598-021-81717-3. Sci Rep. 2021. PMID: 33510204 Free PMC article.
-
Insights from studies of blood substitutes in trauma.Shock. 2005 Sep;24(3):197-205. doi: 10.1097/01.shk.0000180075.76766.fe. Shock. 2005. PMID: 16135956 Review.
-
Hemoglobin-based oxygen carriers for hemorrhagic shock.Resuscitation. 2012 Mar;83(3):285-92. doi: 10.1016/j.resuscitation.2011.09.020. Epub 2011 Oct 5. Resuscitation. 2012. PMID: 21978876 Review.
Cited by
-
Silk Fibroin Particles as Carriers in the Development of Hemoglobin-Based Oxygen Carriers.Adv Nanobiomed Res. 2023 Sep;3(9):2300019. doi: 10.1002/anbr.202300019. Epub 2023 Jul 27. Adv Nanobiomed Res. 2023. PMID: 38708087 Free PMC article.
-
Silk Fibroin Particles as Carriers in the Development of All-Natural Hemoglobin-Based Oxygen Carriers (HBOCs).bioRxiv [Preprint]. 2023 Mar 2:2023.03.01.530637. doi: 10.1101/2023.03.01.530637. bioRxiv. 2023. Update in: Adv Nanobiomed Res. 2023 Sep;3(9):2300019. doi: 10.1002/anbr.202300019. PMID: 36909572 Free PMC article. Updated. Preprint.
-
Veterinary Perspectives on Hemoglobin-Based Oxygen Carriers in Experimental Hemorrhagic Shock: Insights from Rabbit Models.Vet Sci. 2025 May 16;12(5):485. doi: 10.3390/vetsci12050485. Vet Sci. 2025. PMID: 40431578 Free PMC article.
-
Renal glomerular and tubular responses to glutaraldehyde- polymerized human hemoglobin.Front Med (Lausanne). 2023 Jun 13;10:1158359. doi: 10.3389/fmed.2023.1158359. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37384048 Free PMC article.
-
Engineering Synthetic Erythrocytes as Next-Generation Blood Substitutes.Adv Funct Mater. 2024 Jul 10;34(28):2315879. doi: 10.1002/adfm.202315879. Epub 2024 Feb 8. Adv Funct Mater. 2024. PMID: 39386164 Free PMC article.
References
-
- Jones AR, Patel RP, Marques MB, Donnelly JP, Griffin RL, Pittet JF, et al. Older blood is associated with increased mortality and adverse events in massively transfused trauma patients: Secondary analysis of the PROPPR trial. Ann. Emerg. Med. 2019;73(6):650–661. doi: 10.1016/j.annemergmed.2018.09.033. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
