

A scoping review and meta-analysis on the prevalence of pan-tumour biomarkers (dMMR, MSI, high TMB) in different solid tumours
- PMID: 36443366
- PMCID: PMC9705554
- DOI: 10.1038/s41598-022-23319-1
A scoping review and meta-analysis on the prevalence of pan-tumour biomarkers (dMMR, MSI, high TMB) in different solid tumours
Abstract
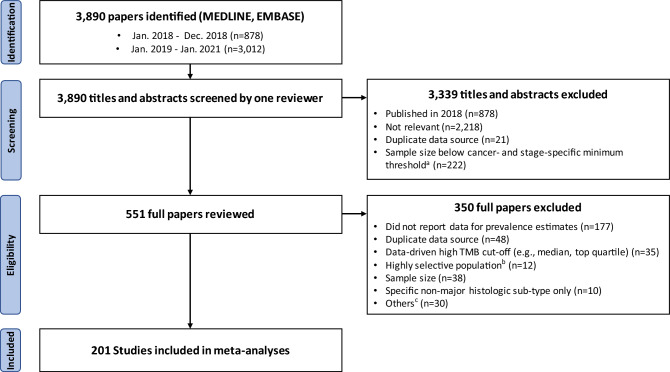
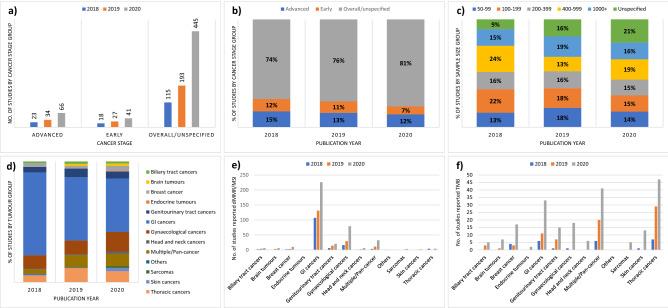
Immune checkpoint inhibitors have been approved in the USA for tumours exhibiting mismatch repair deficiency (dMMR), microsatellite instability (MSI), or high tumour mutational burden (TMB), with regulatory and reimbursement applications in multiple other countries underway. As the estimated budget impacts of future reimbursements depend on the size of the potential target population, we performed a scoping review and meta-analysis of the prevalence of these pan-tumour biomarkers in different cancers. We systematically searched Medline/Embase and included studies reporting the prevalence of dMMR/MSI/high TMB in solid tumours published 01/01/2018-31/01/2021. Meta-analyses were performed separately for the pan-cancer prevalence of each biomarker, and by cancer type and stage where possible. The searches identified 3890 papers, with 433 prevalence estimates for 32 different cancer types from 201 studies included in meta-analyses. The pooled overall prevalence of dMMR, MSI and high TMB (≥ 10 mutations/Mb) in pan-cancer studies was 2.9%, 2.7% and 14.0%, respectively. The prevalence profiles of dMMR/MSI and high TMB differed across cancer types. For example, endometrial, colorectal, small bowel and gastric cancers showed high prevalence of both dMMR and MSI (range: 8.7-26.8% and 8.5-21.9%, respectively) and high TMB (range: 8.5-43.0%), while cervical, esophageal, bladder/urothelial, lung and skin cancers showed low prevalence of dMMR and MSI (< 5%), but high prevalence of high TMB (range: 23.7-52.6%). For other cancer types, prevalence of all three biomarkers was generally low (< 5%). This structured review of dMMR/MSI/high TMB prevalence across cancers and for specific cancer types and stages provide timely evidence to inform budget impact forecasts in health technology assessments for drug approvals based on these pan-tumour biomarkers.
© 2022. The Author(s).
Conflict of interest statement
Professor Karen Canfell is co–principle investigator of an investigator-initiated trial of cervical screening, “Compass”, run by The Australian Centre for the Prevention of Cervical Cancer (ACPCC), which is a government-funded not-for-profit charity; “Compass” receives infrastructure support from the Australian government and the ACPCC has received equipment and a funding contribution from Roche Molecular Diagnostics, USA. She is also co–principle investigator on a major implementation program Elimination of Cervical Cancer in the Western Pacific which has received support from the Minderoo Foundation and the Frazer Family Foundation, and equipment donations from Cepheid Inc. She also receives support for a range of other Australian and international government projects including support from philanthropic organizations, WHO, and government agencies related to cervical cancer control. K.C. is a Chair or member of a number of government or meetings convened by the World Health Organization (WHO), or philanthropic organizations such as Bill and Melinda Gates Foundation (BMGF). Professor John Zalcberg has stock and other ownership interests in Biomarin, Ophthea, Amarin, Concert Pharmaceuticals, Frequency Therapeutics, Gilead, Madrigal Pharmaceuticals, UniQure, Zogenix, rphazyme, Moderna Therapeutics, TWST and Novavax. JZ holds a consulting or advisory role in Merck Serono, Targovax, Merck Sharp & Dohme, Halozyme, Lipotek, Specialized Therapeutics, CEND, Deciphera, REVOLUTION MEDICINE, FivePHusion, Genorbio, 1Global and Novotech. JZ’s institution received funding from Merck Serono, Bristol-Hyers Squibb, AstraZeneca, Pfizer, IQvia, Mylan, Ipsen, Elsai, Medtronic and MSD Oncology. JZ received travel, accommodations and expenses from Merck Serono, AstraZeneca, Merck Sharp & Dohme, Deciphera and Sanofi. Professor Finlay Macrae is a member of the Clinical Advisory Group of the National Bowel Cancer Screening Program. His group receives support from Cancer Australia and the Victorian Cancer Agency for Australian leadership of the CAPP trials for cancer prevention in Lynch Syndrome. He chairs the Australian and New Zealand Gastrointestinal International Training Association which receives support from industry, philanthropic organizations and Australian Government for its activities in the Indo-Pacific region. He is the principal investigator of several clinical trials funded by the pharmaceutical industry. Other authors do not have competing interest.
Figures
Similar articles
-
ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: a systematic review-based approach.Ann Oncol. 2019 Aug 1;30(8):1232-1243. doi: 10.1093/annonc/mdz116. Ann Oncol. 2019. PMID: 31056702
-
Mutational analysis of microsatellite-stable gastrointestinal cancer with high tumour mutational burden: a retrospective cohort study.Lancet Oncol. 2023 Feb;24(2):151-161. doi: 10.1016/S1470-2045(22)00783-5. Epub 2023 Jan 18. Lancet Oncol. 2023. PMID: 36681091 Free PMC article.
-
Microsatellite Instability, Tumor Mutational Burden, and Response to Immune Checkpoint Blockade in Patients with Prostate Cancer.Clin Cancer Res. 2024 Sep 3;30(17):3894-3903. doi: 10.1158/1078-0432.CCR-23-3403. Clin Cancer Res. 2024. PMID: 38949888 Free PMC article.
-
Tumour mutational burden as a biomarker in patients with mismatch repair deficient/microsatellite instability-high metastatic colorectal cancer treated with immune checkpoint inhibitors.Eur J Cancer. 2023 Jul;187:15-24. doi: 10.1016/j.ejca.2023.03.029. Epub 2023 Mar 31. Eur J Cancer. 2023. PMID: 37099945
-
Tumor Mutational Burden Predicting the Efficacy of Immune Checkpoint Inhibitors in Colorectal Cancer: A Systematic Review and Meta-Analysis.Front Immunol. 2021 Sep 29;12:751407. doi: 10.3389/fimmu.2021.751407. eCollection 2021. Front Immunol. 2021. PMID: 34659255 Free PMC article.
Cited by
-
Nationwide Real-World Data of Microsatellite Instability and/or Mismatch Repair Deficiency in Cancer: Prevalence and Testing Patterns.Diagnostics (Basel). 2024 May 22;14(11):1076. doi: 10.3390/diagnostics14111076. Diagnostics (Basel). 2024. PMID: 38893603 Free PMC article.
-
Tumor-Agnostic Precision Medicine from the AACR GENIE Database: Clinical Implications.Clin Cancer Res. 2023 Aug 1;29(15):2753-2760. doi: 10.1158/1078-0432.CCR-23-0090. Clin Cancer Res. 2023. PMID: 37061987 Free PMC article.
-
PFMG2025-integrating genomic medicine into the national healthcare system in France.Lancet Reg Health Eur. 2025 Jan 6;50:101183. doi: 10.1016/j.lanepe.2024.101183. eCollection 2025 Mar. Lancet Reg Health Eur. 2025. PMID: 40093400 Free PMC article. Review.
-
Tissue-agnostic biomarkers in solid tumors: current approvals and emerging candidates.Cancer Metastasis Rev. 2025 Jun 27;44(3):58. doi: 10.1007/s10555-025-10274-2. Cancer Metastasis Rev. 2025. PMID: 40576713 Free PMC article. Review.
-
Neoadjuvant PD-1 blockade: a new treatment option for patients with early-stage mismatch repair deficient solid tumors.J Immunother Cancer. 2025 Aug 25;13(8):e013061. doi: 10.1136/jitc-2025-013061. J Immunother Cancer. 2025. PMID: 40854816 Free PMC article.
References
-
- U.S. Food & Drug Administration. FDA News release: FDA approves first cancer treatment for any solid tumor with a specific genetic feature. https://www.fda.gov/news-events/press-announcements/fda-approves-first-c.... Accessed 21 October 2020.
-
- Therapeutic Goods Administration. Prescription medicines: new or extended uses, or new combinations of registered medicines, 2019. https://www.tga.gov.au/prescription-medicines-new-or-extended-uses-or-ne.... Accessed 21 October 2020.
-
- Merck Receives Positive EU CHMP Opinion for KEYTRUDA® (pembrolizumab) as First-Line Treatment in Adult Patients With Metastatic Microsatellite Instability-High (MSI-H) or Mismatch Repair Deficient (dMMR) Colorectal Cancer. https://www.merck.com/news/merck-receives-positive-eu-chmp-opinion-for-k.... Accessed 23 December 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
