

Quantification of bowel ischaemia using real-time multispectral Single Snapshot Imaging of Optical Properties (SSOP)
- PMID: 36443562
- PMCID: PMC10017661
- DOI: 10.1007/s00464-022-09764-z
Quantification of bowel ischaemia using real-time multispectral Single Snapshot Imaging of Optical Properties (SSOP)
Abstract
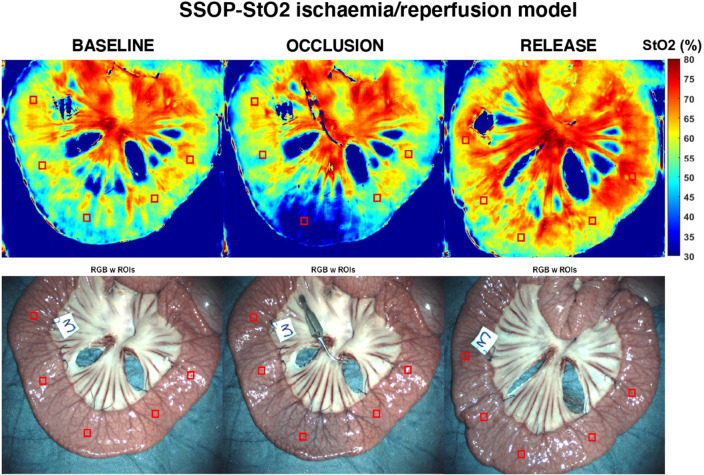
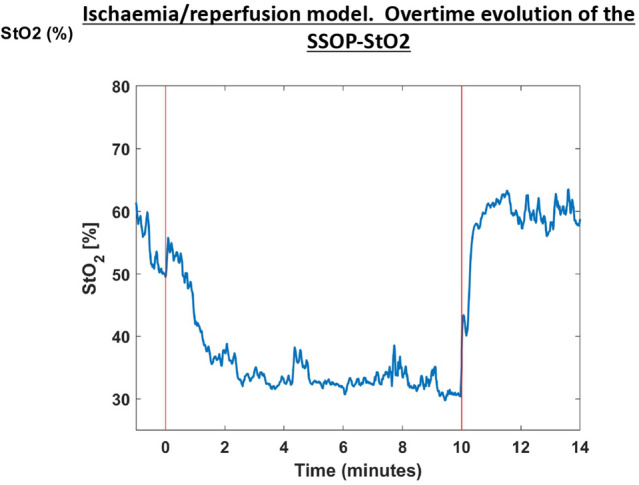
Background: Single snapshot imaging of optical properties (SSOP) is a relatively new non-invasive, real-time, contrast-free optical imaging technology, which allows for the real-time quantitative assessment of physiological properties, including tissue oxygenation (StO2). This study evaluates the accuracy of multispectral SSOP in quantifying bowel ischaemia in a preclinical experimental model.
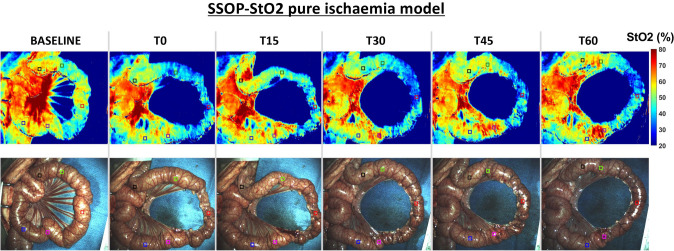
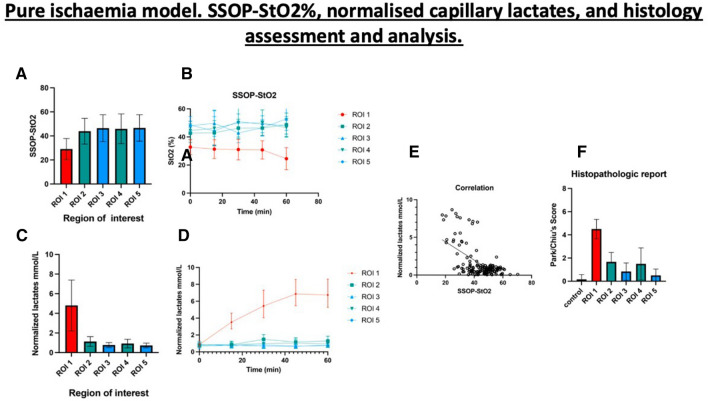
Methods: In six pigs, an ischaemic bowel segment was created by dividing the arcade branches. Five regions of interest (ROIs) were identified on the bowel loop, as follows: ROI 1: central ischaemic; ROI 2: left marginal; ROI 3: left vascularised; ROI 4: right marginal; and ROI 5: right vascularised. The Trident imaging system, specifically developed for real-time tissue oxygenation imaging using SSOP, was used to image before (T0) and after ischaemia induction. Capillary and systemic lactates were measured at each time point (T0, T15, T30, T45, T60), as well as StO2 values acquired by means of SSOP (SSOP-StO2).
Results: The mean value of SSOP-StO2 in ROI 1 was 30.08 ± 6.963 and was significantly lower when compared to marginal ROIs (ROI 2 + ROI 4: 45.67 ± 10.02 p = < 0.0001), and to vascularised ROIs (ROI 3 + ROI 5: 48.08 ± 7.083 p = < 0.0001). SSOP-StO2 was significantly correlated with normalised lactates r = - 0.5892 p < 0.0001 and with histology r =- 0.6251 p = 0.0002.
Conclusion: Multispectral SSOP allows for a contrast-free accurate assessment of small bowel perfusion identifying physiological tissue oxygenation as confirmed with perfusion biomarkers.
Keywords: Anastomotic leak; Diffuse optical imaging; Image-guided surgery; Single snapshot imaging of optical properties; Tissue perfusion.
© 2022. The Author(s).
Conflict of interest statement
Sylvain Gioux and Luca Baratelli are employees of Intuitive Surgical Sàrl. Jacques Marescaux is the President of the IRCAD, which is partly funded by KARL STORZ and Medtronic. María Rita Rodríguez-Luna was supported by the following project grant: European Union’s Horizon 2020 research and innovation programme, under the Marie Skłodowska-Curie grant agreement No. 857894 – CAST. Drs. Nariaki Okamoto, Lorenzo Cinelli, Silvère Ségaud, Adriana Rodríguez-Gómez, Deborah S. Keller, Elisa Bannone, Michele Diana, and Ms. Elham Zonoobi have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi: 10.1097/01.sla.0000133083.54934.ae. - DOI - PMC - PubMed
-
- Frasson M, Flor-Lorente B, Rodríguez JLR, Granero-Castro P, Hervás D, Alvarez Rico MA, et al. Risk factors for anastomotic leak after colon resection for cancer: Multivariate analysis and nomogram from a multicentric, prospective, national study with 3193 patients. Ann Surg. 2015;262(2):321–330. doi: 10.1097/SLA.0000000000000973. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
