

Low QRS Voltages in Cardiac Amyloidosis: Clinical Correlates and Prognostic Value
- PMID: 36444225
- PMCID: PMC9700257
- DOI: 10.1016/j.jaccao.2022.08.007
Low QRS Voltages in Cardiac Amyloidosis: Clinical Correlates and Prognostic Value
Abstract
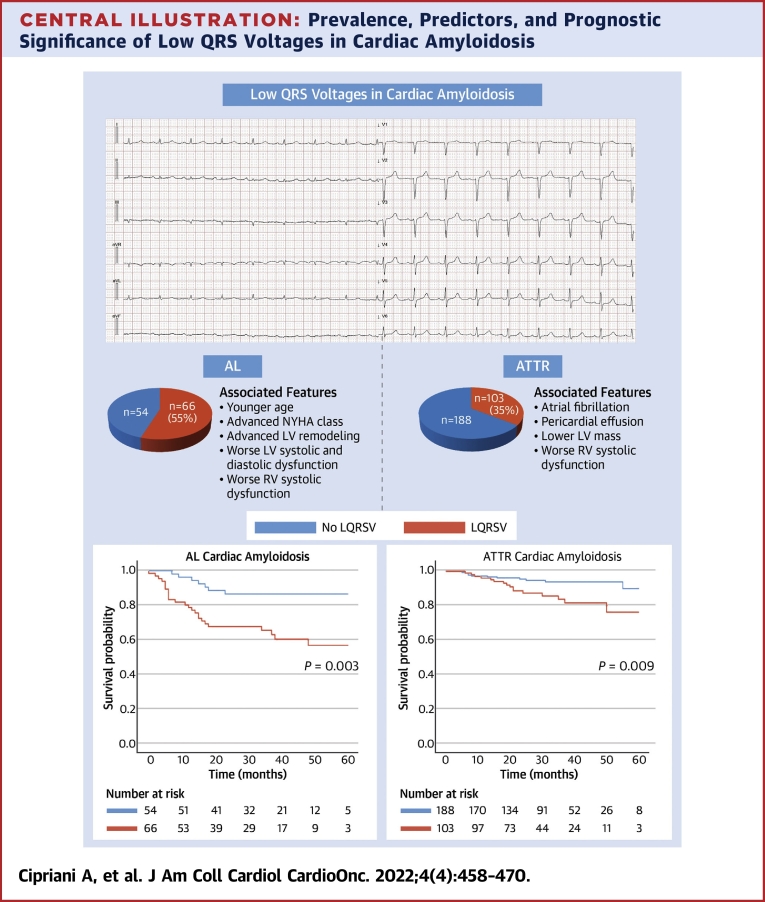
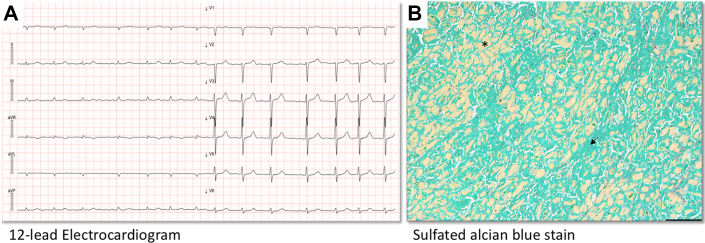
Background: Low QRS voltages (LQRSVs) are a common electrocardiographic feature in patients with light chain amyloidosis (AL) and transthyretin amyloidosis (ATTR) cardiac amyloidosis (CA).
Objectives: The aim of this study was to identify clinical and echocardiographic correlates of LQRSV and to investigate their prognostic significance in patients with CA.
Methods: This was a multicenter, retrospective study performed in 6 CA referral centers including consecutive patients with AL and ATTR CA. LQRSVs were defined as a QRS amplitude ≤5 mm (0.5 mV) in all peripheral leads. The study outcome was cardiovascular (CV) mortality.
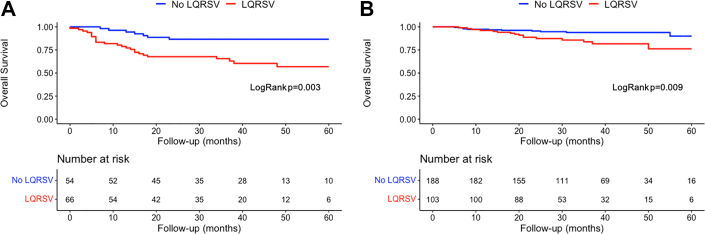
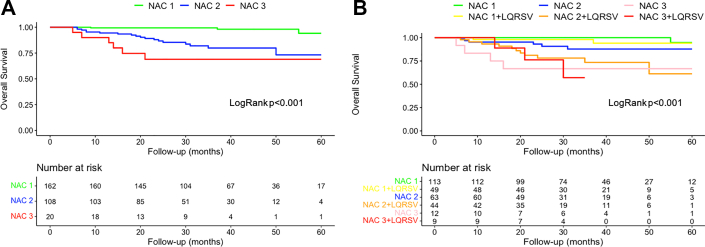
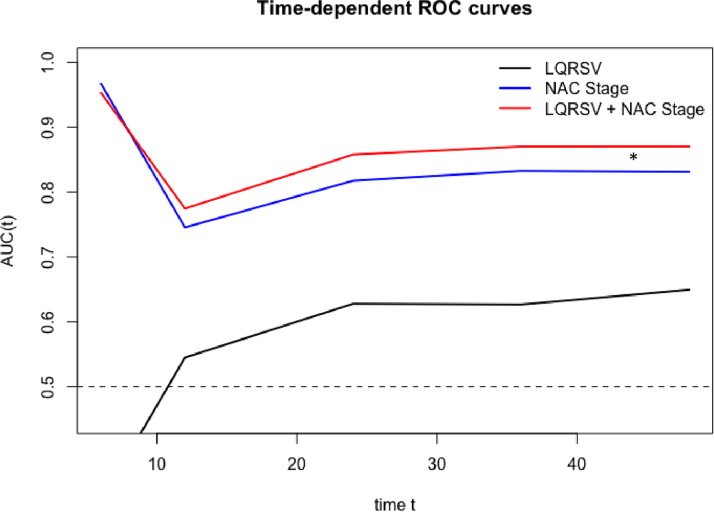
Results: Overall, 411 (AL CA: n = 120, ATTR CA: n = 291) patients were included. LQRSVs were present in 66 (55%) patients with AL CA and 103 (35%) with ATTR CA (P < 0.001). In AL CA, LQRSVs were independently associated with younger age (P = 0.015), higher New York Heart Association functional class (P = 0.016), and natriuretic peptides (P = 0.041); in ATTR CA, LQRSVs were independently associated with pericardial effusion (P = 0.008) and lower tricuspid annulus peak systolic excursion (P = 0.038). During a median follow-up of 33 months (Q1-Q3: 21-46), LQRSVs independently predicted CV death in both AL CA (HR: 1.76; 95% CI: 2.41-10.18; P = 0.031) and ATTR CA (HR: 2.64; 95% CI: 1.82-20.17; P = 0.005). Together with the National Amyloidosis Centre (NAC) staging, LQRSVs provided incremental prognostic value in ATTR CA (AUC for NAC model: 0.83 [95% CI: 0.77-0.89]; AUC for NAC + LQRSV model: 0.87 [95% CI: 0.81-0.93]; P = 0.040).
Conclusions: LQRSVs are common but not ubiquitous in CA; they are more frequent in AL CA than in ATTR CA. LQRSVs reflect an advanced disease stage and independently predict CV death. In ATTR CA, LQRSVs can provide incremental prognostic accuracy over the NAC staging system in patients with intermediate risk.
Keywords: AL, light chain amyloidosis; ATTR, transthyretin amyloidosis; ATTR-v, variant transthyretin; ATTR-wt, wild-type transthyretin; AUC, area under the curve; BNP, B-type natriuretic peptide; CA, cardiac amyloidosis; CMR, cardiac magnetic resonance; CV, cardiovascular; ECG, electrocardiogram; LQRSV, low QRS voltages; LV, left ventricle; LVEDD, left ventricular end-diastolic diameter; NAC, National Amyloidosis Centre; NT-proBNP, N-terminal pro–B-type natriuretic peptide; NYHA, New York Heart Association; ROC, receiver-operating characteristic; RV, right ventricular; TAPSE, tricuspid annulus peak systolic excursion; cardiac amyloidosis; echocardiography; electrocardiography; low QRS voltages; prognostic significance; risk stratification.
© 2022 The Authors.
Conflict of interest statement
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
