

10-Year Temporal Trends of In-Hospital Mortality and Emergency Percutaneous Coronary Intervention for Acute Myocardial Infarction
- PMID: 36444314
- PMCID: PMC9700040
- DOI: 10.1016/j.jacasi.2022.06.005
10-Year Temporal Trends of In-Hospital Mortality and Emergency Percutaneous Coronary Intervention for Acute Myocardial Infarction
Abstract
Background: The mortality rate of acute myocardial infarction (AMI) has improved dramatically because of reperfusion therapy during the last 40 years; however, recent temporal trends for AMI have not been fully clarified in Japan.
Objectives: The purpose of this study was to elucidate the temporary trend in in-hospital mortality and treatment of AMI for the last decade in the Tokyo Metropolitan area.
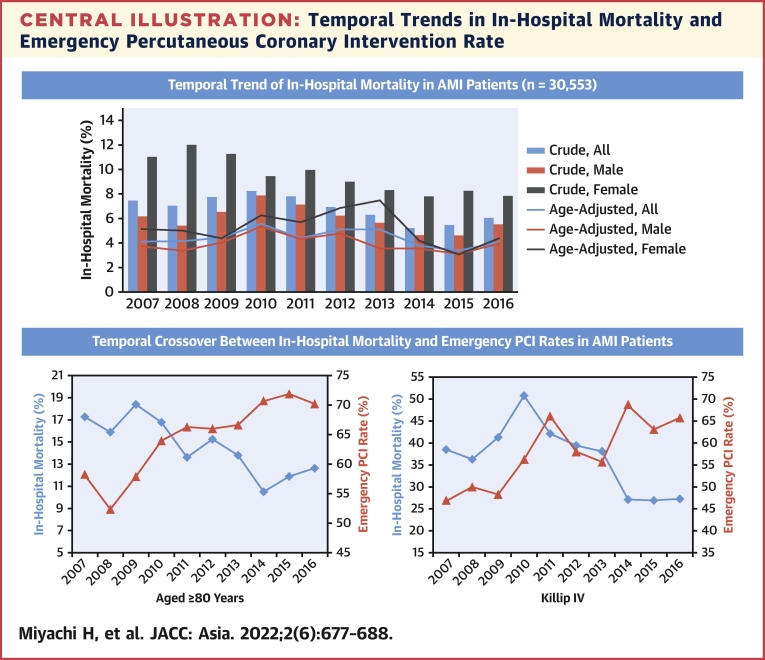
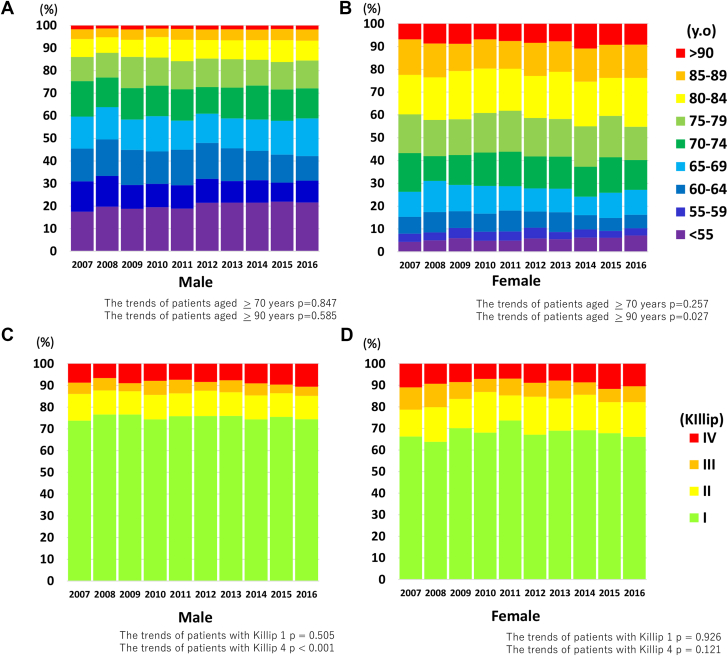
Methods: We enrolled 30,553 patients from the Tokyo Cardiovascular Care Unit Network Registry, diagnosed with AMI from 2007 to 2016, as part of an ongoing, multicenter, cohort study. We analyzed the temporal trends in basic characteristics, treatment, and in-hospital mortality of AMI.
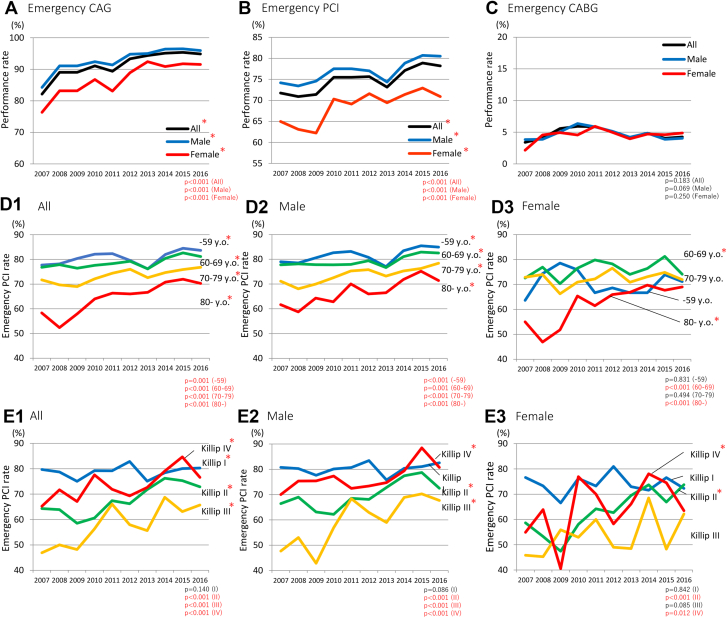
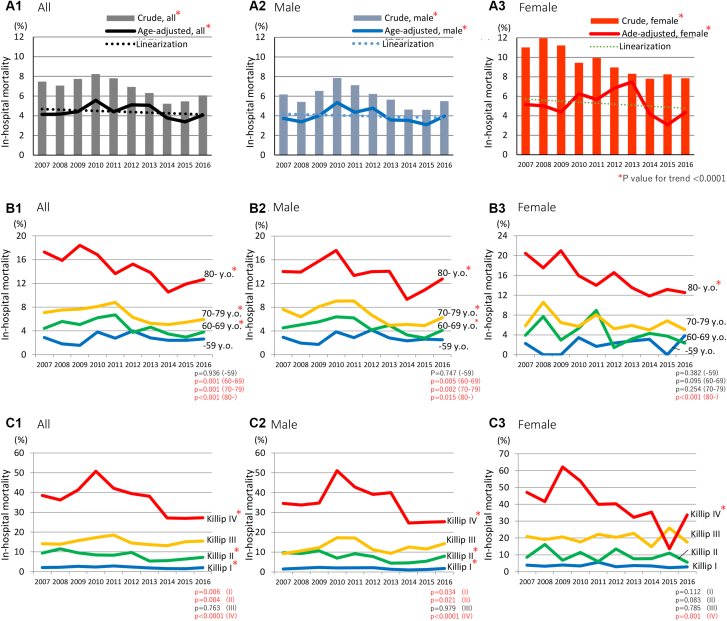
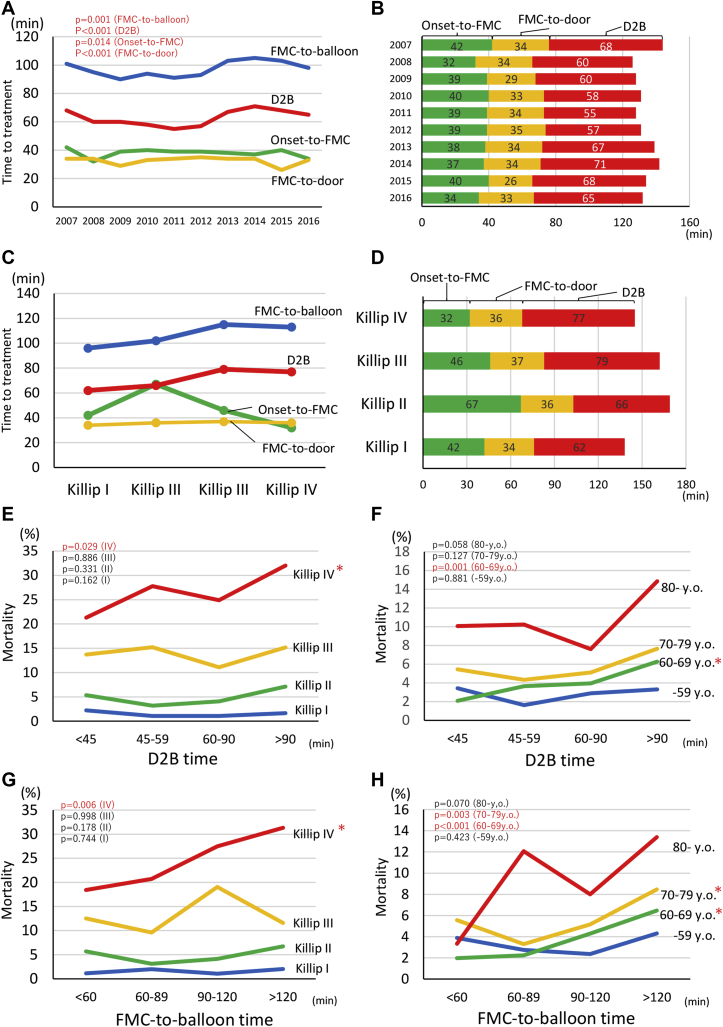
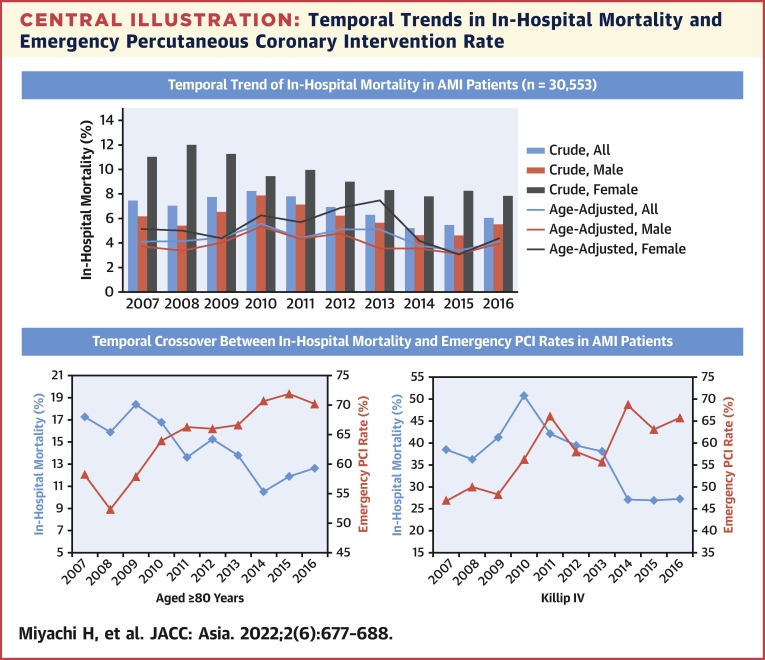
Results: The overall emergency percutaneous coronary intervention (PCI) rate significantly increased (P < 0.001). In particular, it remarkably increased in patients older than 80 years of age (58.3% to 70.3%, P < 0.001) and patients with Killip III or IV (Killip III, 46.9% to 65.7%; Killip IV, 65.2% to 76.6%, P < 0.001 for both). The crude and age-adjusted in-hospital mortality remained low (5.2% to 8.2% and 3.4% to 5.5%, respectively) and significantly decreased during the decade (P < 0.001). The in-hospital mortality remarkably decreased in patients older than 80 years of age (17.3% to 12.7%, P < 0.001) and in those with cardiogenic shock (38.5% to 27.3%, P < 0.001).
Conclusions: This large cohort study from Tokyo revealed that in-hospital mortality of AMI significantly decreased with the increase in emergency percutaneous coronary intervention rate over the decade, particularly for high-risk patients such as older patients and those with cardiogenic shock.
Keywords: AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; CAG, coronary angiography; CCU, cardiovascular care unit; D2B, door to balloon; ECMO, extracorporeal membrane oxygenation; FMC, first medical contact; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; in-hospital mortality; older patients; percutaneous coronary intervention; sex; temporal trends.
© 2022 The Authors.
Conflict of interest statement
The Tokyo CCU network database for this study was financially supported by the Tokyo Metropolitan Government. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
Identifying and Solving Gaps in Pre- and In-Hospital Acute Myocardial Infarction Care in Asia-Pacific Countries.Korean Circ J. 2023 Sep;53(9):594-605. doi: 10.4070/kcj.2023.0169. Korean Circ J. 2023. PMID: 37653695 Free PMC article. Review.
-
Current characteristics and management of ST elevation and non-ST elevation myocardial infarction in the Tokyo metropolitan area: from the Tokyo CCU network registered cohort.Heart Vessels. 2016 Nov;31(11):1740-1751. doi: 10.1007/s00380-015-0791-9. Epub 2016 Jan 12. Heart Vessels. 2016. PMID: 26758733 Free PMC article.
-
Implementation of extracorporeal membrane oxygenation before primary percutaneous coronary intervention may improve the survival of patients with ST-segment elevation myocardial infarction and refractory cardiogenic shock.Int J Cardiol. 2018 Oct 15;269:45-50. doi: 10.1016/j.ijcard.2018.07.023. Epub 2018 Jul 7. Int J Cardiol. 2018. PMID: 30077527
-
Acute myocardial infarction-cardiogenic shock in patients with prior coronary artery bypass grafting: A 16-year national cohort analysis of temporal trends, management and outcomes.Int J Cardiol. 2020 Jul 1;310:9-15. doi: 10.1016/j.ijcard.2020.02.033. Epub 2020 Feb 13. Int J Cardiol. 2020. PMID: 32085862
-
In-Hospital Mortality in Patients With Acute Myocardial Infarction: A Literature Overview.Cureus. 2024 Aug 12;16(8):e66729. doi: 10.7759/cureus.66729. eCollection 2024 Aug. Cureus. 2024. PMID: 39268294 Free PMC article. Review.
Cited by
-
Mechanical circulatory support in cardiogenic shock.J Intensive Care. 2023 Dec 19;11(1):64. doi: 10.1186/s40560-023-00710-2. J Intensive Care. 2023. PMID: 38115065 Free PMC article. Review.
-
Population-Based Trends in Complexity of Hospital Inpatients.JAMA Intern Med. 2024 Feb 1;184(2):183-192. doi: 10.1001/jamainternmed.2023.7410. JAMA Intern Med. 2024. PMID: 38190179 Free PMC article.
-
Sex Differences in DeBakey Type I/II Acute Aortic Dissection Outcomes: The Tokyo Acute Aortic Super-network.JACC Adv. 2023 Oct 30;2(9):100661. doi: 10.1016/j.jacadv.2023.100661. eCollection 2023 Nov. JACC Adv. 2023. PMID: 38938720 Free PMC article.
-
CVIT expert consensus document on primary percutaneous coronary intervention (PCI) for acute coronary syndromes (ACS) in 2024.Cardiovasc Interv Ther. 2024 Oct;39(4):335-375. doi: 10.1007/s12928-024-01036-y. Epub 2024 Sep 20. Cardiovasc Interv Ther. 2024. PMID: 39302533 Free PMC article.
-
Identifying and Solving Gaps in Pre- and In-Hospital Acute Myocardial Infarction Care in Asia-Pacific Countries.Korean Circ J. 2023 Sep;53(9):594-605. doi: 10.4070/kcj.2023.0169. Korean Circ J. 2023. PMID: 37653695 Free PMC article. Review.
References
-
- Virani S.S., Alonso A., Aparicio H.J., et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143:e254–e743. - PubMed
-
- Szummer K., Wallentin L., Lindhagen L., et al. Improved outcomes in patients with ST-elevation myocardial infarction during the last 20 years are related to implementation of evidence-based treatments: experiences from the SWEDEHEART registry 1995-2014. Eur Heart J. 2017;38:3056–3065. - PMC - PubMed
-
- Long-term care, health and welfare services for the elderly. Ministry of Health, Labour and Welfare. Government of Japan. https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/...
-
- Cui Y., Hao K., Takahashi J., et al. Age-specific trends in the incidence and in-hospital mortality of acute myocardial infarction over 30 years in Japan — report from the Miyagi AMI Registry Study. Circ J. 2017;81:520–528. - PubMed
-
- Kojima S., Matsui K., Ogawa H. Temporal trends in hospitalization for acute myocardial infarction between 2004 and 2011 in Kumamoto, Japan. Circ J. 2013;77:2841–2843. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
