

Prognostic Impact of Systemic Coagulation-Inflammation Index in Acute Type A Aortic Dissection Surgery
- PMID: 36444319
- PMCID: PMC9700012
- DOI: 10.1016/j.jacasi.2022.06.007
Prognostic Impact of Systemic Coagulation-Inflammation Index in Acute Type A Aortic Dissection Surgery
Abstract
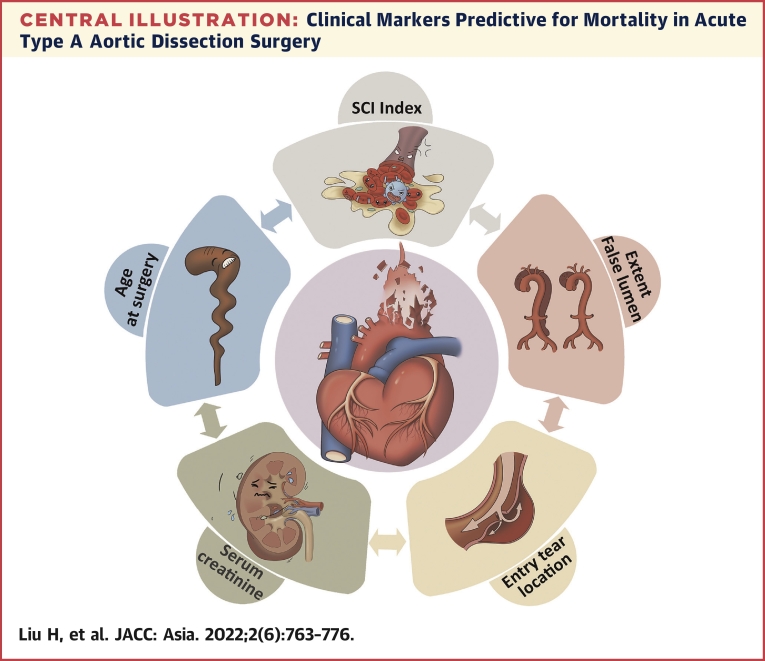
Background: A novel hematologic parameter, systemic coagulation-inflammation (SCI) index reflecting inflammation and coagulation pathways could be easily obtained from clinically routine laboratory findings. We hypothesize that the SCI index has prognostic implication in predicting operative mortality for patients with acute type A aortic dissection (ATAAD).
Objectives: This study aims to investigate the prognostic value of the SCI index and to establish an SCI-adding nomogram for mortality prediction in ATAAD patients.
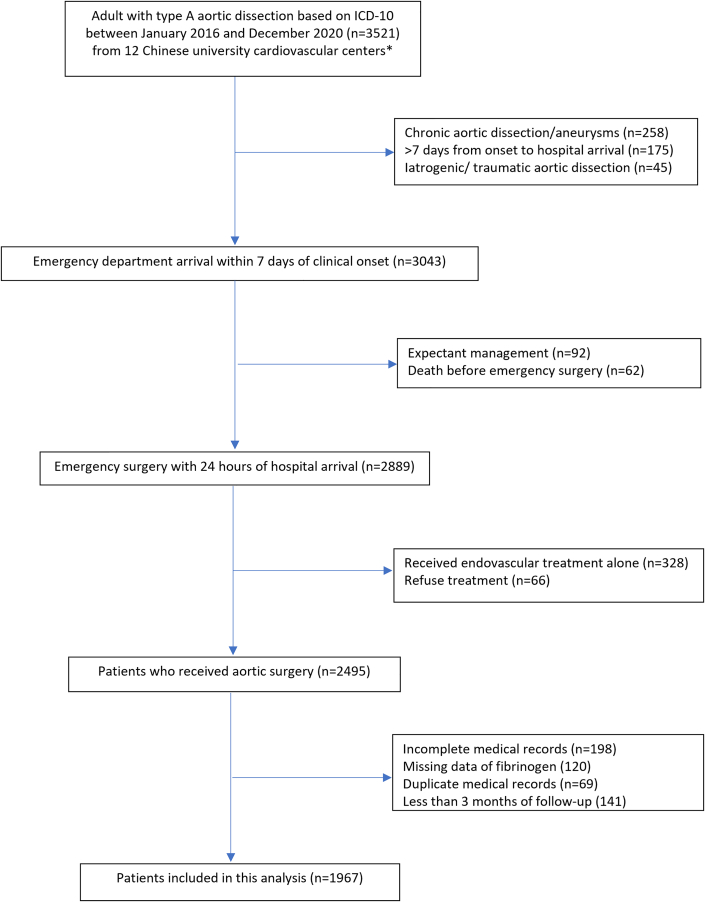
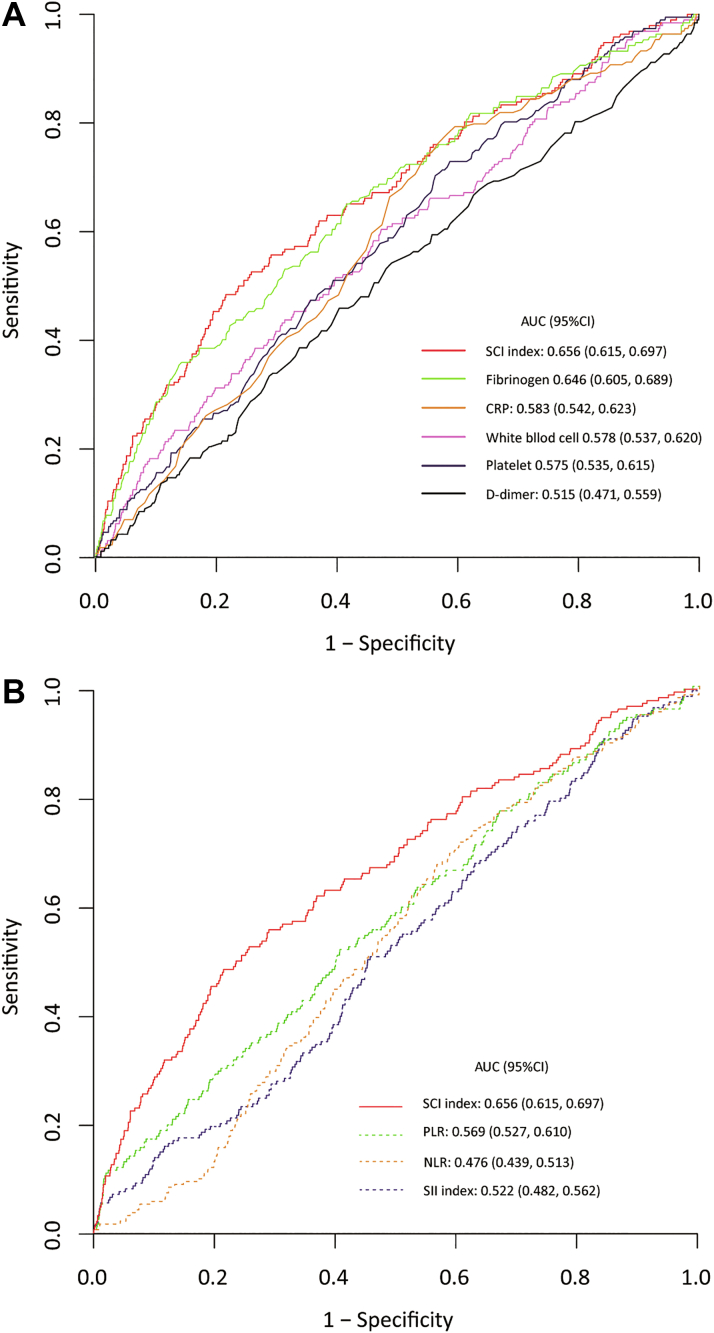
Methods: A total of 1,967 ATAAD patients surgically repaired were collected from 12 Chinese cardiovascular centers by the 5A (Additive Anti-inflammatory Action for Aortopathy & Arteriopathy [Multicenter Retrospective Study]) study III (2016-2020). SCI index was calculated as platelet count × fibrinogen/white blood cell count on admission. By adding SCI index, a nomogram was developed and evaluated for 90-day mortality prediction with conventional predictors via the Cox model with 10-fold cross-validation.
Results: Patients were stratified with low SCI (<40), middle SCI (40-100), or high SCI (>100). The 90-day survival rates increased with SCI index (low 86.9%; [95% CI: 84.9%-89.0%], middle 92.7% [95% CI: 90.9%-94.9%], and high 96.4% [95% CI: 94.2%-98.6%]; log-rank P < 0.001). SCI index is independently associated with 90-day mortality (adjusted hazard ratio: 0.549; 95% CI: 0.424-0.710; P < 0.001). The addition of SCI index provided significantly incremental prognostic value to base model including age, serum creatinine, DeBakey class, and location of intimal entry (area under the curve: 0.677; 95% CI: 0.641-0.716 vs 0.724; 95% CI: 0.685-0.760; P = 0.002), which was confirmed by net reclassification improvement index (0.158; 95% CI: 0.065-0.235; P < 0.001) and integrated discrimination improvement index (0.070; 95% CI: 0.007-0.036; P < 0.001).
Conclusions: SCI index is easily obtainable, performs moderately well as a predictor of short-term mortality in ATAAD patients, and may be useful for risk stratification in emergency settings. (Additive Anti-inflammatory Action for Aortopathy & Arteriopathy [Multicenter Retrospective Study] III NCT04918108).
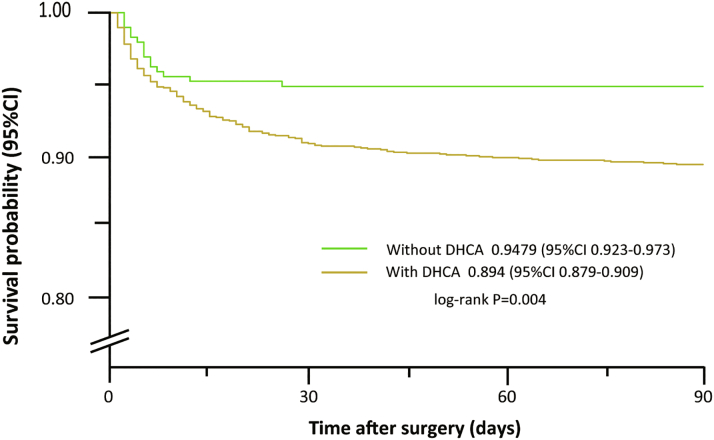
Keywords: ATAAD, acute type A aortic dissection; AUC, the area under the curve; DHCA, deep hypothermic circulatory arrest; SCI, systemic coagulation-inflammation index; SII, systemic immune-inflammation index; coagulation; inflammation; mortality; type A aortic dissection.
© 2022 The Authors.
Conflict of interest statement
This work was supported by the National Natural Science Foundation of China (82000305, 82070483), Scientific Research Common Program of Beijing Municipal Commission of Education (KM202110025014), and Beijing Municipal Science and Technology Commission (Z211100002921010). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Erbel R., Aboyans V., Boileau C., et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The task force for the diagnosis and treatment of aortic diseases of the European Society of Cardiology (ESC) Eur Heart J. 2014;35(41):2873–2926. - PubMed
-
- Bossone E., Eagle K.A. Epidemiology and management of aortic disease: aortic aneurysms and acute aortic syndromes. Nat Rev Cardiol. 2021;18(5):331–348. - PubMed
-
- Morello F., Cavalot G., Giachino F., et al. White blood cell and platelet count as adjuncts to standard clinical evaluation for risk assessment in patients at low probability of acute aortic syndrome. Eur Heart J Acute Cardiovasc Care. 2017;6(5):389–395. - PubMed
-
- Zindovic I., Sjögren J., Bjursten H., et al. The coagulopathy of acute type A aortic dissection: a prospective, observational study. J Cardiothorac Vasc Anesth. 2019;33(10):2746–2754. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
