

COVID-19 subphenotypes at hospital admission are associated with mortality: a cross-sectional study
- PMID: 36444856
- PMCID: PMC10795648
- DOI: 10.1080/07853890.2022.2148733
COVID-19 subphenotypes at hospital admission are associated with mortality: a cross-sectional study
Abstract
Background: We have an incomplete understanding of COVID-19 characteristics at hospital presentation and whether underlying subphenotypes are associated with clinical outcomes and therapeutic responses.
Methods: For this cross-sectional study, we extracted electronic health data from adults hospitalized between 1 March and 30 August 2020 with a PCR-confirmed diagnosis of COVID-19 at five New York City Hospitals. We obtained clinical and laboratory data from the first 24 h of the patient's hospitalization. Treatment with tocilizumab and convalescent plasma was assessed over hospitalization. The primary outcome was mortality; secondary outcomes included intubation, intensive care unit (ICU) admission and length of stay (LOS). First, we employed latent class analysis (LCA) to identify COVID-19 subphenotypes on admission without consideration of outcomes and assigned each patient to a subphenotype. We then performed robust Poisson regression to examine associations between COVID-19 subphenotype assignment and outcome. We explored whether the COVID-19 subphenotypes had a differential response to tocilizumab and convalescent plasma therapies.
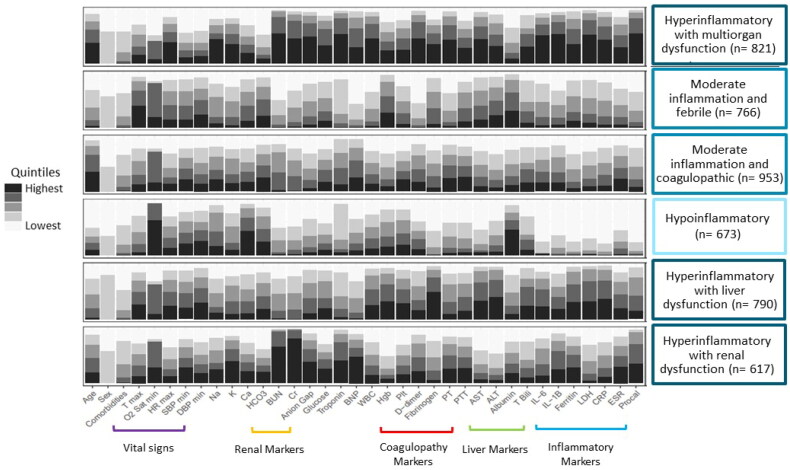
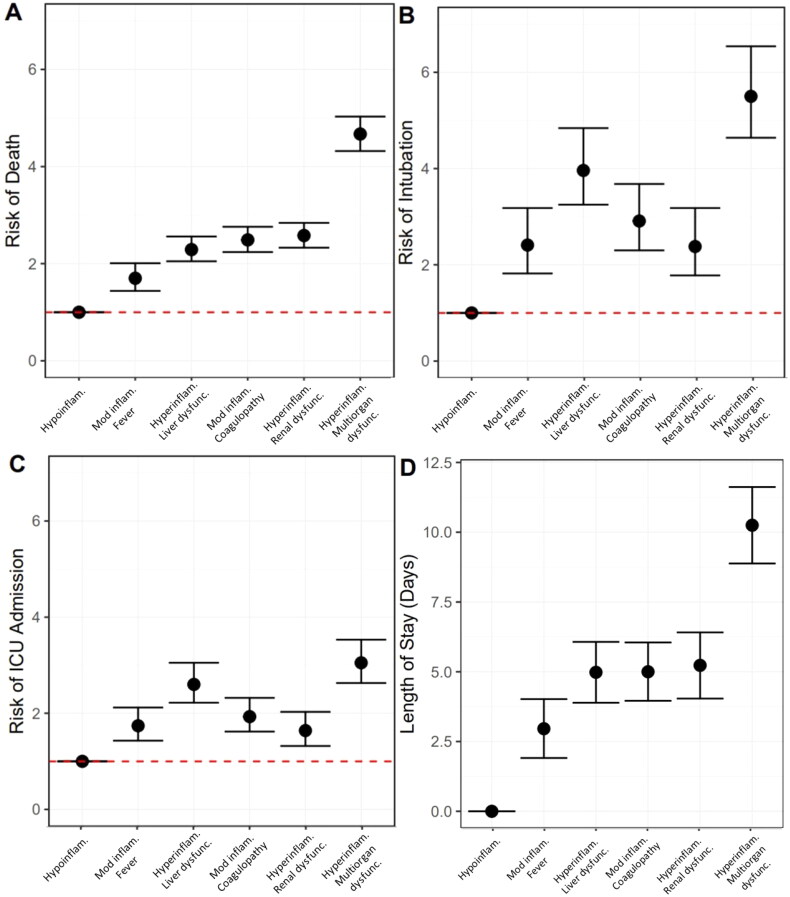
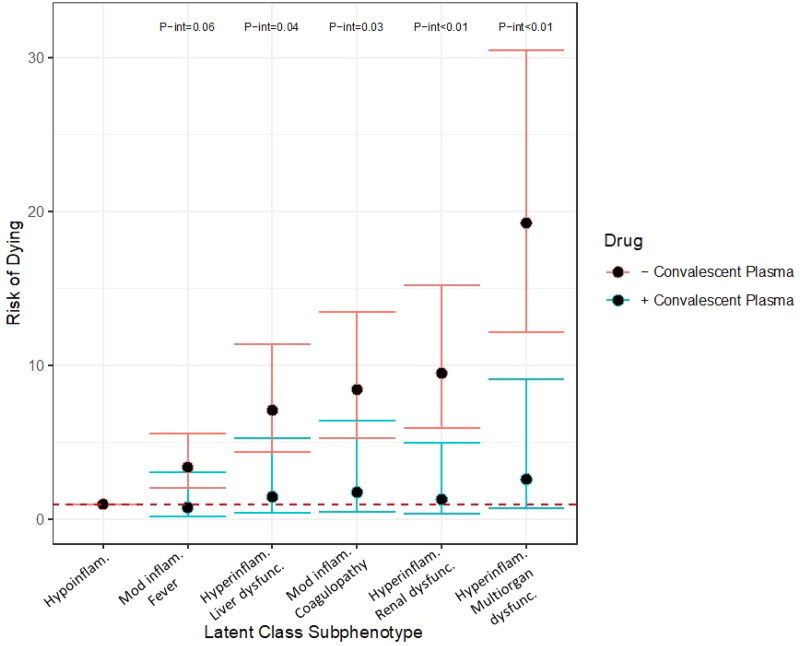
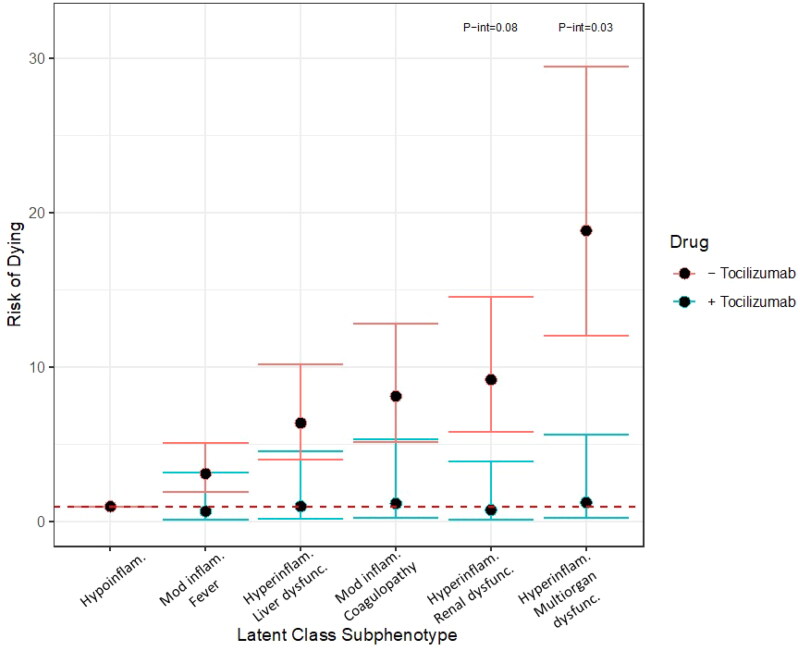
Results: A total of 4620 patients were included. LCA identified six subphenotypes, which were distinct by level of inflammation, clinical and laboratory derangements and ranged from a hypoinflammatory subphenotype with the fewest derangements to a hyperinflammatory with multiorgan dysfunction subphenotypes. Multivariable regression analyses found differences in risk for mortality, intubation, ICU admission and LOS, as compared to the hypoinflammatory subphenotype. For example, in multivariable analyses the moderate inflammation with fever subphenotype had 3.29 times the risk of mortality (95% CI 2.05, 5.28), while the hyperinflammatory with multiorgan failure subphenotype had 17.87 times the risk of mortality (95% CI 11.56, 27.63), as compared to the hypoinflammatory subphenotype. Exploratory analyses suggested that subphenotypes may differential respond to convalescent plasma or tocilizumab therapy.
Conclusion: COVID-19 subphenotype at hospital admission may predict risk for mortality, ICU admission and intubation and differential response to treatment.KEY MESSAGEThis cross-sectional study of COVID patients admitted to the Mount Sinai Health System, identified six distinct COVID subphenotypes on admission. Subphenotypes correlated with ICU admission, intubation, mortality and differential response to treatment.
Keywords: COVID-19; SARS CoV-2 infection; mortality; subphenotypes.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Centers for Disease Control and Prevention [CDC] . Estimated Disease Burden of COVID-19. 2020; [cited 2021 April 20]; Available from: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burden.html
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous