

Efficacy and Safety of Melatonin as Prophylaxis for Migraine in Adults: A Meta-analysis
- PMID: 36445912
- PMCID: PMC10586587
- DOI: 10.11607/ofph.3211
Efficacy and Safety of Melatonin as Prophylaxis for Migraine in Adults: A Meta-analysis
Abstract
Aims: To evaluate the efficacy and safety of melatonin for migraine prophylaxis in adults.
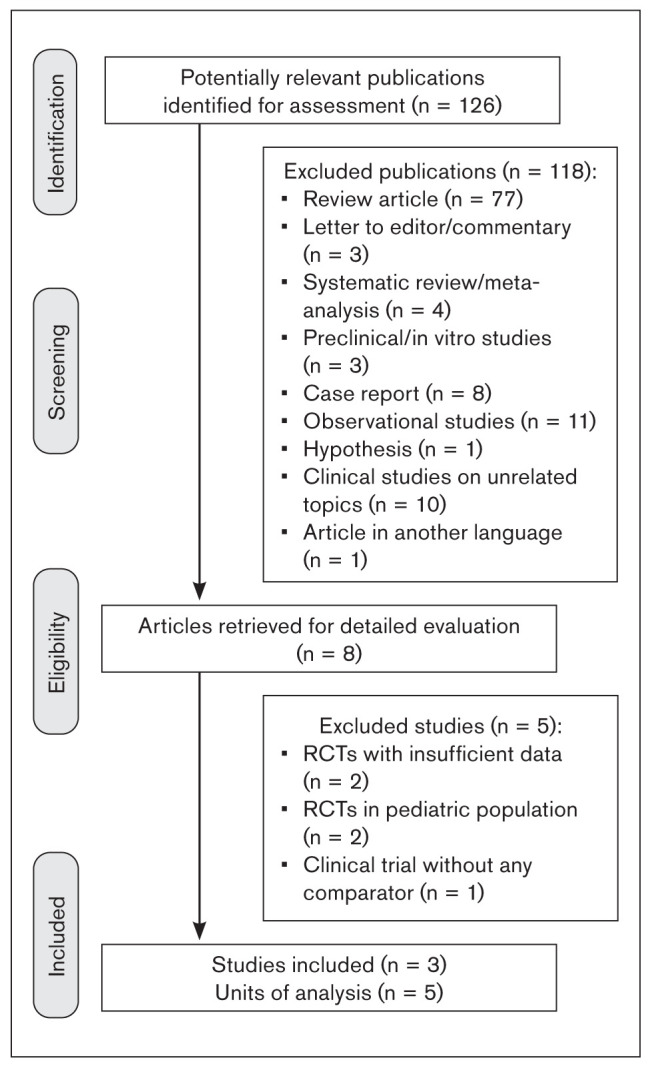
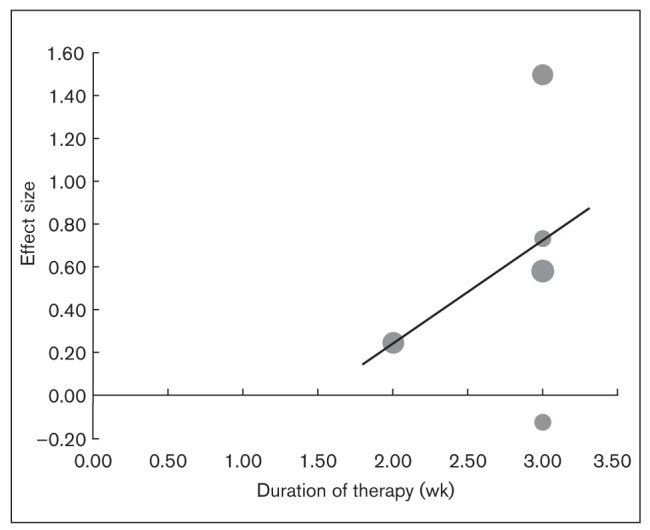
Methods: After a comprehensive literature search in the MEDLINE, Cochrane Database, and International Clinical Trial Registry Platform databases, reviewers extracted data from three relevant articles. PRISMA guidelines were followed in the selection, analysis, and reporting of the findings. Quality assessment was performed using the Cochrane risk of bias assessment tool. A random-effects model was used to estimate the effect size, and meta-regression was performed for variables with a likely influence on effect size. Subgroup analysis was performed based on the comparison used in the included studies.
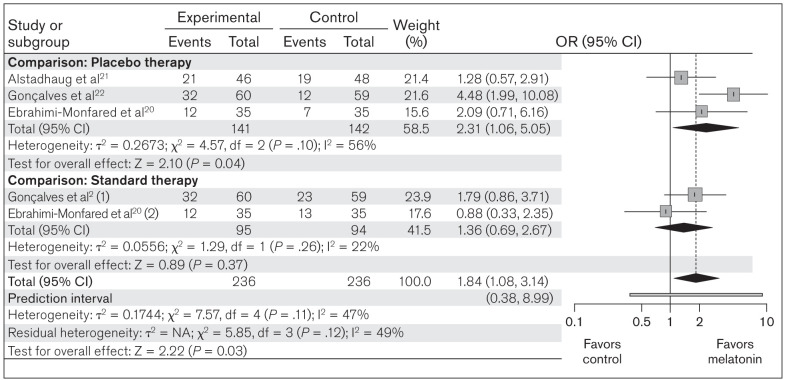
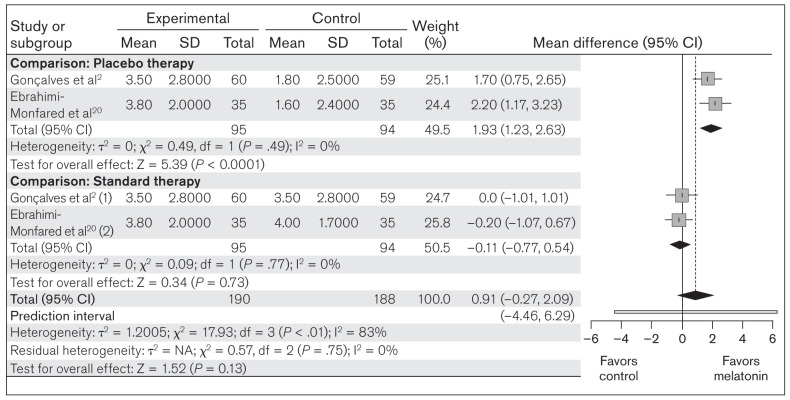
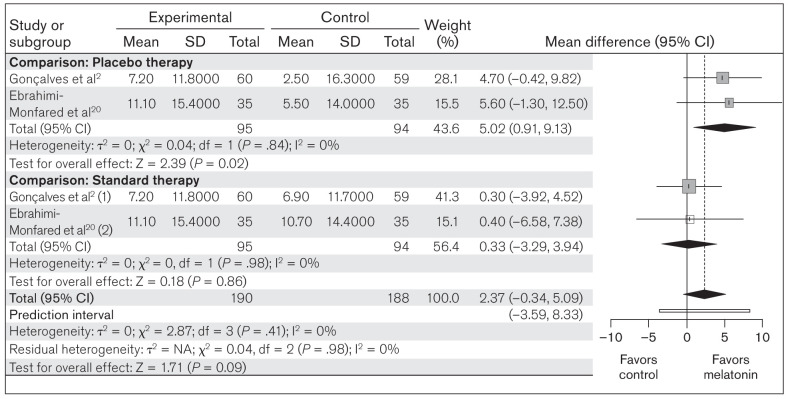
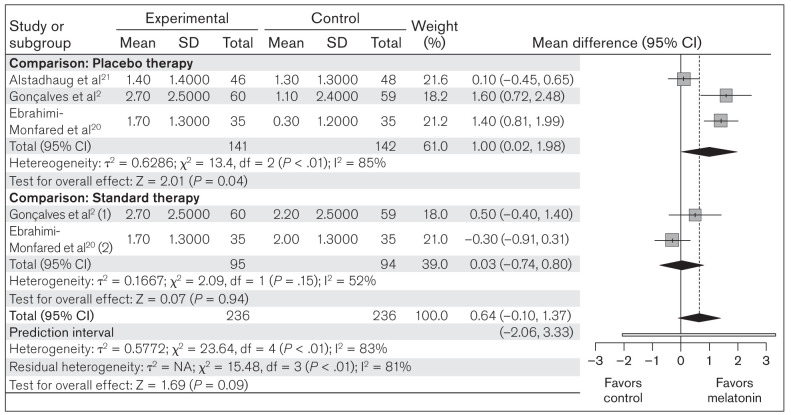
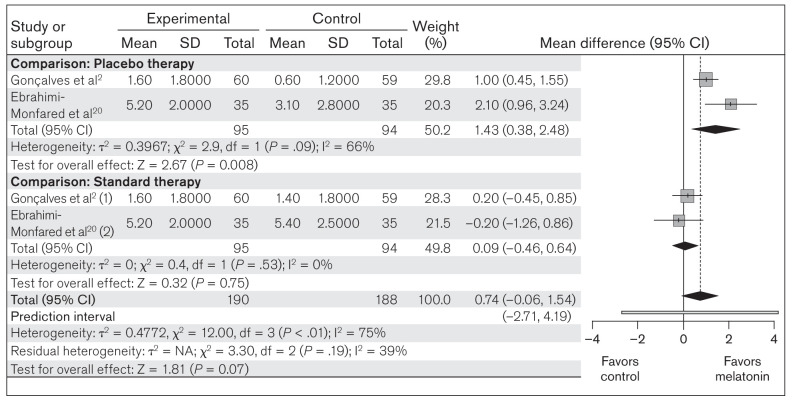
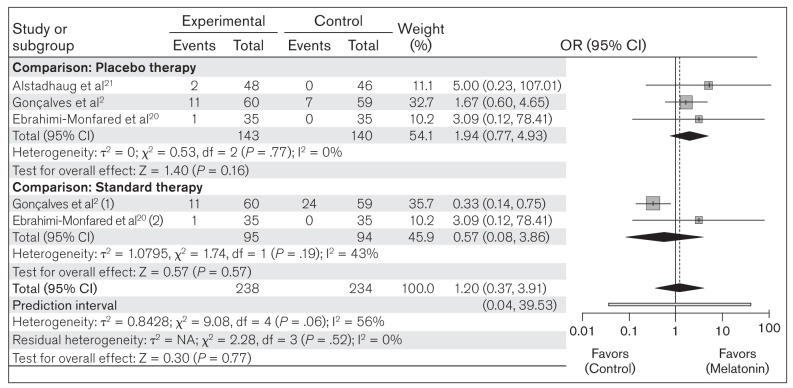
Results: Melatonin therapy in migraine was associated with a significantly higher responder rate when compared to both placebo and standard therapy (OR = 1.84; 95% CI: 1.08 to 3.14; P = .03). The results of the meta-analyses indicated that melatonin can achieve a significant reduction in frequency of migraine attacks (MD = 1.00; 95% CI: 0.02 to 1.98; P = .04), migraine attack duration (MD = 5.02; 95% CI: 0. 91 to 9.13; P = .02), use of analgesics (MD = 1.43; 95% CI: 0.38 to 2.48; P = .008), and migraine severity (MD = 1.93; 95% CI: 1.23 to 2.63; P < .0001) over placebo, but had no significant effects in comparison to amitriptyline or valproate. There was no significant difference in the occurrence of common adverse drug reactions, such as drowsiness and fatigue, between the melatonin group and the comparison groups.
Conclusions: Melatonin showed a beneficial prophylactic role in migraine, with a better responder rate in comparison to placebo in reducing migraine severity, mean attack duration, mean attack frequency, and analgesic use, but did not show significant effects in comparison to amitriptyline or valproate.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Endogenous Melatonin Levels and Therapeutic Use of Exogenous Melatonin in Migraine: Systematic Review and Meta-Analysis.Headache. 2020 Jul;60(7):1273-1299. doi: 10.1111/head.13828. Epub 2020 Apr 30. Headache. 2020. PMID: 32352572
-
Use of melatonin versus valproic acid in prophylaxis of migraine patients: A double-blind randomized clinical trial.Restor Neurol Neurosci. 2017;35(4):385-393. doi: 10.3233/RNN-160704. Restor Neurol Neurosci. 2017. PMID: 28800342 Clinical Trial.
-
Randomised clinical trial comparing melatonin 3 mg, amitriptyline 25 mg and placebo for migraine prevention.J Neurol Neurosurg Psychiatry. 2016 Oct;87(10):1127-32. doi: 10.1136/jnnp-2016-313458. Epub 2016 May 10. J Neurol Neurosurg Psychiatry. 2016. PMID: 27165014 Free PMC article. Clinical Trial.
-
The Effect of Melatonin on Reducing the Frequency and Severity of Migraine Attacks: A Double-Blind, Randomized Clinical Trial.Iran J Med Sci. 2024 May 1;49(5):313-321. doi: 10.30476/ijms.2023.97782.2965. eCollection 2024 May. Iran J Med Sci. 2024. PMID: 38751874 Free PMC article. Clinical Trial.
-
Efficacy and Safety of Lasmiditan for Acute Treatment of Migraine in Adults: A Meta-Analysis.J Clin Pharmacol. 2021 Dec;61(12):1534-1544. doi: 10.1002/jcph.1962. Epub 2021 Nov 12. J Clin Pharmacol. 2021. PMID: 34472095 Review.
Cited by
-
Melatonin treatment has consistent but transient beneficial effects on sleep measures and pain in patients with severe chronic pain: the DREAM-CP randomised controlled trial.Br J Anaesth. 2024 Apr;132(4):725-734. doi: 10.1016/j.bja.2024.01.012. Epub 2024 Feb 14. Br J Anaesth. 2024. PMID: 38355388 Free PMC article. Clinical Trial.
-
Serum melatonin levels and in a sample of Iranian patients with migraine.Sci Rep. 2024 Oct 2;14(1):22883. doi: 10.1038/s41598-024-73278-y. Sci Rep. 2024. Retraction in: Sci Rep. 2025 Jan 28;15(1):3548. doi: 10.1038/s41598-025-87562-y. PMID: 39358369 Free PMC article. Retracted.
-
Apparent resolution of hypersomnia episodes in two patients with Kleine-Levin syndrome following treatment with the melatonin receptor agonist ramelteon.J Clin Sleep Med. 2024 Apr 1;20(4):657-662. doi: 10.5664/jcsm.10968. J Clin Sleep Med. 2024. PMID: 38156412 Free PMC article.
-
The effectiveness of agomelatine on headache severity and frequency in episodic migraine without aura; a parallel randomized controlled trial study.BMC Neurol. 2024 Jan 2;24(1):2. doi: 10.1186/s12883-023-03516-9. BMC Neurol. 2024. PMID: 38166859 Free PMC article. Clinical Trial.
References
-
- Buse DC, Manack A, Serrano D, Turkel C, Lipton RB. Sociodemographic and comorbidity profiles of chronic migraine and episodic migraine sufferers. J Neurol Neurosurg Psychiatry. 2010;81:428–432. - PubMed
-
- Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68:343–349. - PubMed
-
- Silberstein SD, Holland S, Freitag F, et al. Evidence-based guideline update: Pharmacologic treatment for episodic migraine prevention in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology. 2012;78:1337–1345. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
