

Training with noninvasive brain-machine interface, tactile feedback, and locomotion to enhance neurological recovery in individuals with complete paraplegia: a randomized pilot study
- PMID: 36446797
- PMCID: PMC9709065
- DOI: 10.1038/s41598-022-24864-5
Training with noninvasive brain-machine interface, tactile feedback, and locomotion to enhance neurological recovery in individuals with complete paraplegia: a randomized pilot study
Abstract
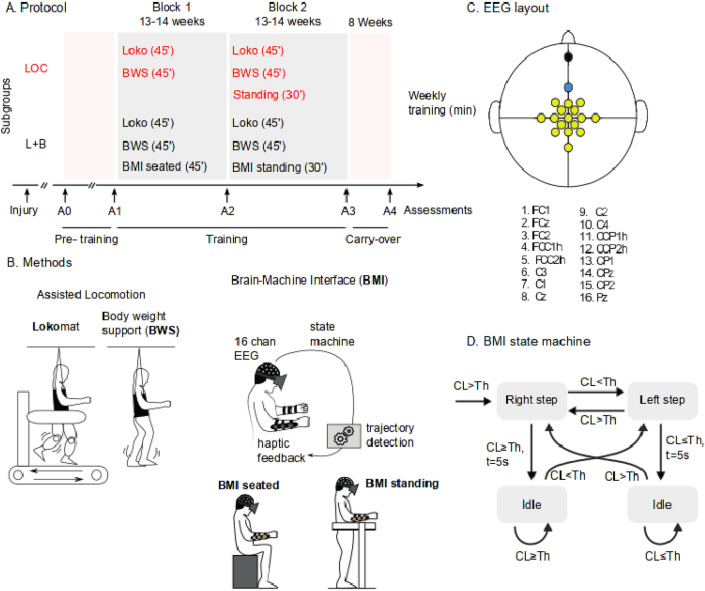
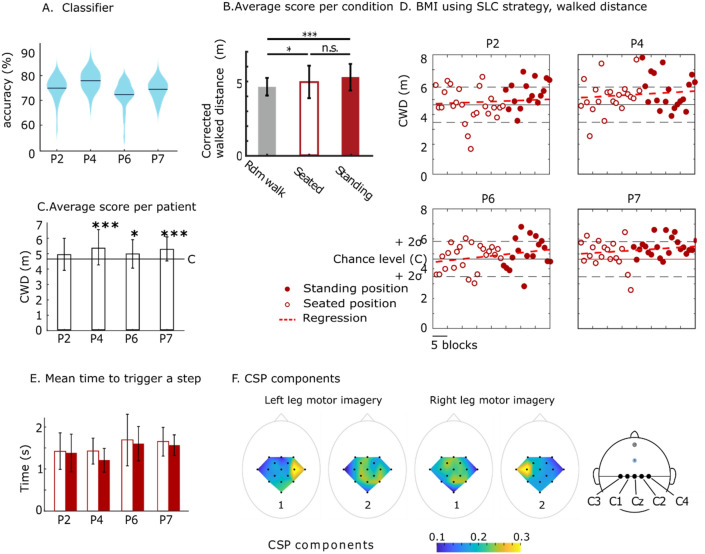
In recent years, our group and others have reported multiple cases of consistent neurological recovery in people with spinal cord injury (SCI) following a protocol that integrates locomotion training with brain machine interfaces (BMI). The primary objective of this pilot study was to compare the neurological outcomes (motor, tactile, nociception, proprioception, and vibration) in both an intensive assisted locomotion training (LOC) and a neurorehabilitation protocol integrating assisted locomotion with a noninvasive brain-machine interface (L + BMI), virtual reality, and tactile feedback. We also investigated whether individuals with chronic-complete SCI could learn to perform leg motor imagery. We ran a parallel two-arm randomized pilot study; the experiments took place in São Paulo, Brazil. Eight adults sensorimotor-complete (AIS A) (all male) with chronic (> 6 months) traumatic spinal SCI participated in the protocol that was organized in two blocks of 14 weeks of training and an 8-week follow-up. The participants were allocated to either the LOC group (n = 4) or L + BMI group (n = 4) using block randomization (blinded outcome assessment). We show three important results: (i) locomotion training alone can induce some level of neurological recovery in sensorimotor-complete SCI, and (ii) the recovery rate is enhanced when such locomotion training is associated with BMI and tactile feedback (∆Mean Lower Extremity Motor score improvement for LOC = + 2.5, L + B = + 3.5; ∆Pinprick score: LOC = + 3.75, L + B = + 4.75 and ∆Tactile score LOC = + 4.75, L + B = + 9.5). (iii) Furthermore, we report that the BMI classifier accuracy was significantly above the chance level for all participants in L + B group. Our study shows potential for sensory and motor improvement in individuals with chronic complete SCI following a protocol with BMIs and locomotion therapy. We report no dropouts nor adverse events in both subgroups participating in the study, opening the possibility for a more definitive clinical trial with a larger cohort of people with SCI.Trial registration: http://www.ensaiosclinicos.gov.br/ identifier RBR-2pb8gq.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- World Health Organization. The International Spinal Cord Society . International Perspectives on Spinal Cord Injury. World Health Organization; 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
