

Learning curve and surgical outcome of robotic assisted colorectal surgery with ERAS program
- PMID: 36446802
- PMCID: PMC9709162
- DOI: 10.1038/s41598-022-24665-w
Learning curve and surgical outcome of robotic assisted colorectal surgery with ERAS program
Abstract
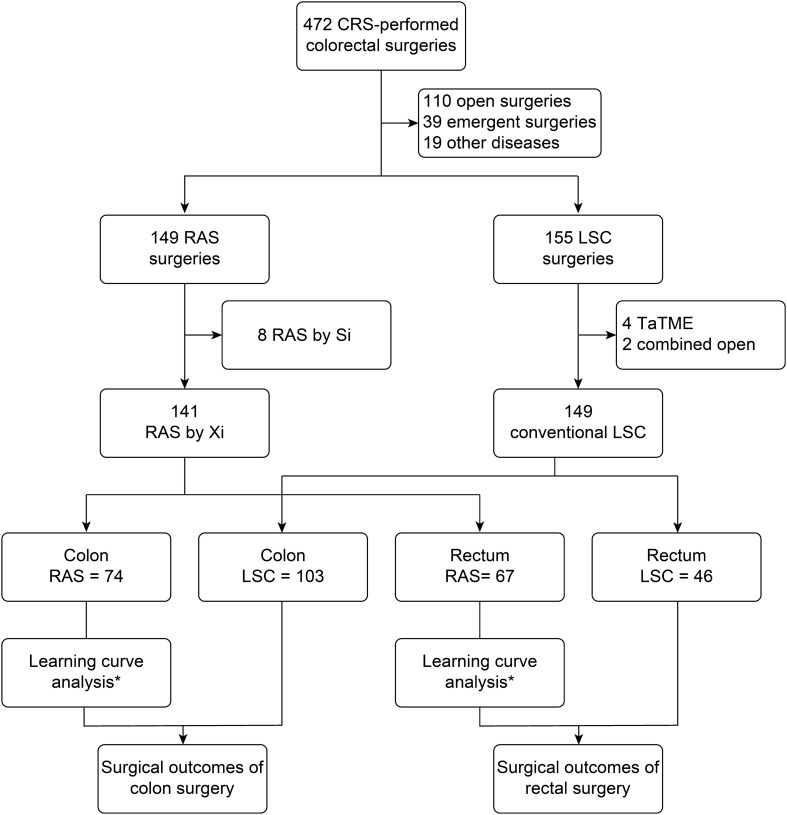
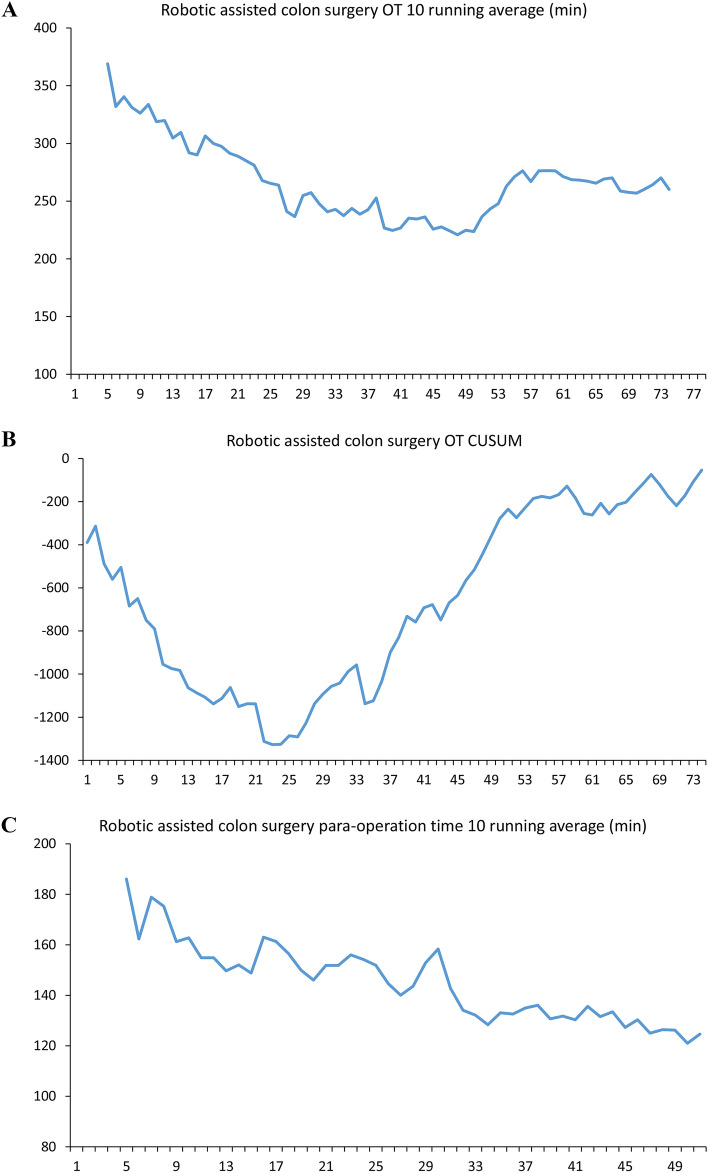
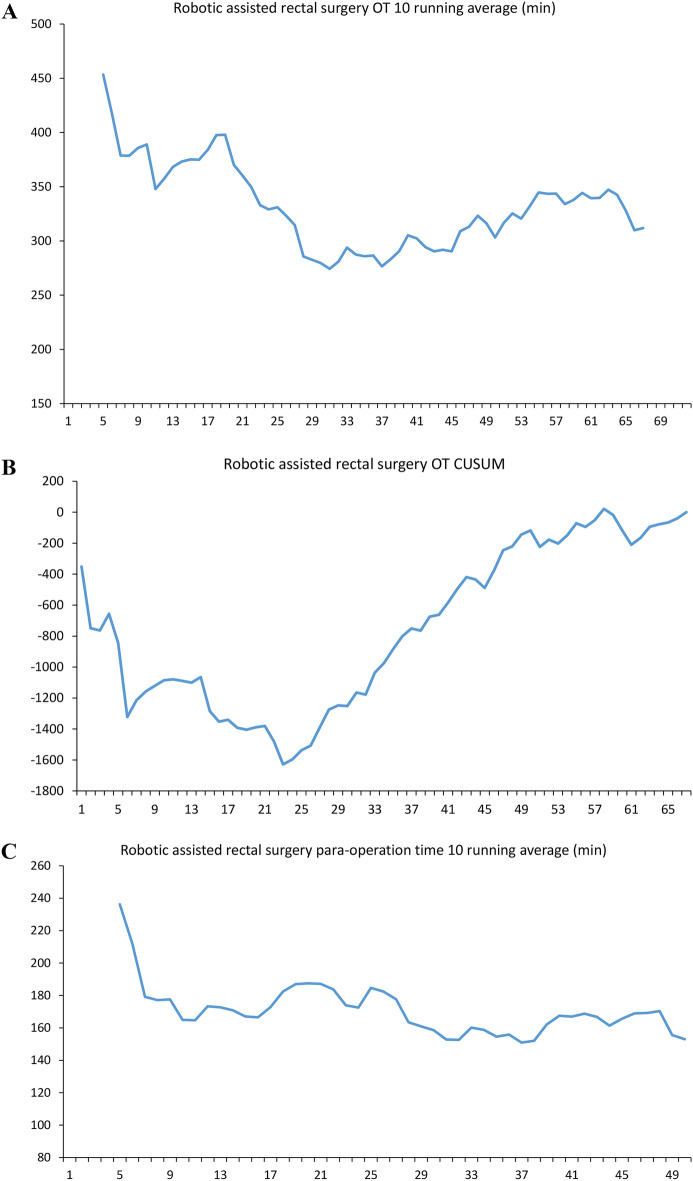
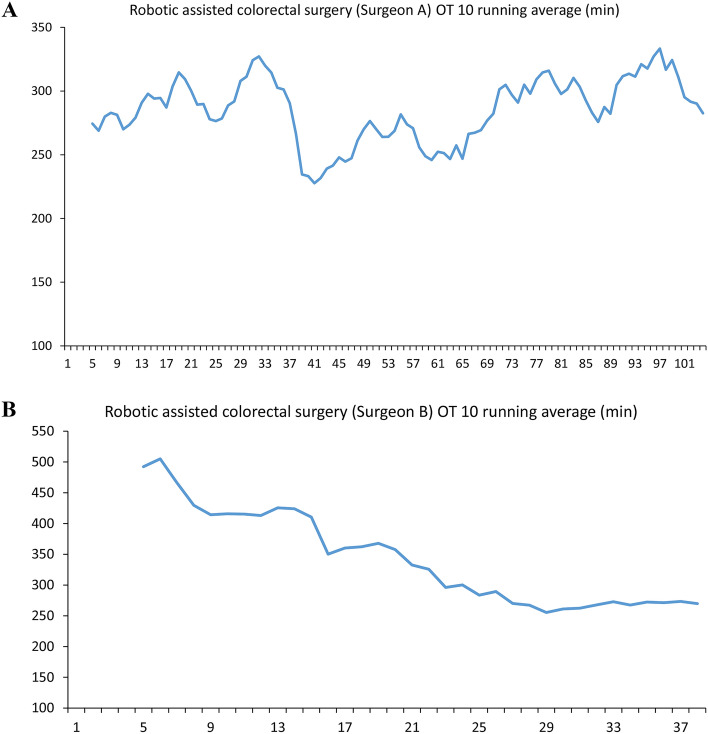
This study analyzed learning curve and the surgical outcome of robotic assisted colorectal surgery with ERAS program. The study results serve as a reference for future robotic colorectal surgeon who applied ERAS in clinical practice. This was a retrospective case-control study to analyze the learning curve of 141 robotic assisted colorectal surgery (RAS) by Da Vinci Xi (Xi) system and compare the surgical outcomes with 147 conventional laparoscopic (LSC) surgery in the same team. Evaluation for maturation was performed by operation time and the CUSUM plot. Patients were recruited from 1st February 2019 to 9th January 2022; follow-up was conducted at 30 days, and the final follow-up was conducted on 9th February 2022. It both took 31 cases for colon and rectal robotic surgeries to reach the maturation phase. Teamwork maturation was achieved after 60 cases. In the maturation stage, RAS required a longer operation time (mean: colon: 249.5 ± 46.5 vs. 190.3 ± 57.3 p < 0.001; rectum 314.9 ± 59.6 vs. 223.6 ± 63.5 p < 0.001). After propensity score matching, robotic surgery with ERAS program resulted in significant shorter length of hospital stay (mean: colon: 5.5 ± 4.5 vs. 10.0 ± 11.9, p < 0.001; rectum: 5.4 ± 3.5 vs. 10.1 ± 7.0, p < 0.001), lower minor complication rate (colon: 6.0% vs 20.0%, p = 0.074 ; rectum: 11.1% vs 33.3%, p = 0.102), and no significant different major complication rate (colon: 2.0% vs 6.0%, p = 0.617; rectum: 7.4% cs 7.4%, p = 1.0) to conventional LSC. Learning curve for robotic assisted colorectal surgery takes 31 cases. Robotic surgery with ERAS program brings significant faster recovery and fewer complication rate compared to laparoscopy in colorectal surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
