

Efficiency of TB service provision in the public and private health sectors in Ethiopia
- PMID: 36447315
- PMCID: PMC9728951
- DOI: 10.5588/ijtld.21.0481
Efficiency of TB service provision in the public and private health sectors in Ethiopia
Abstract
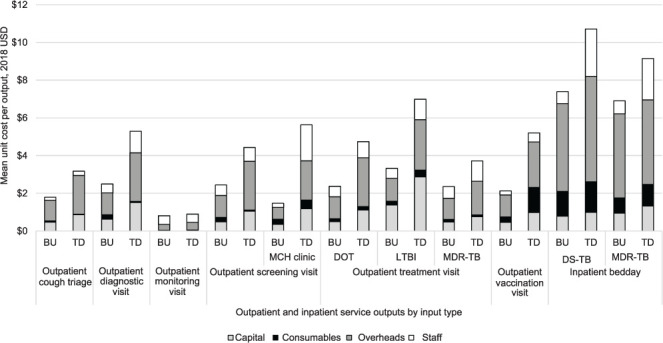
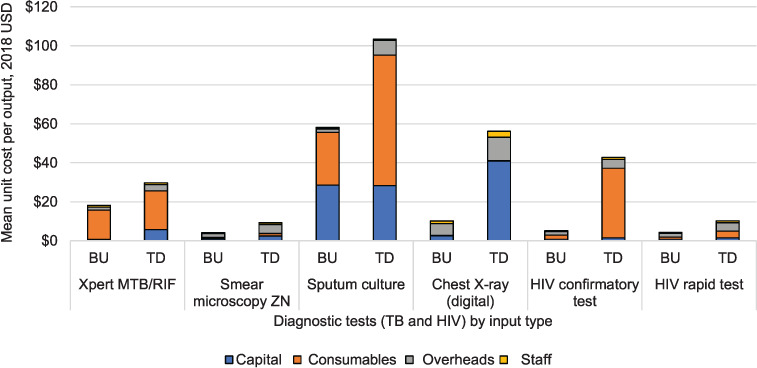
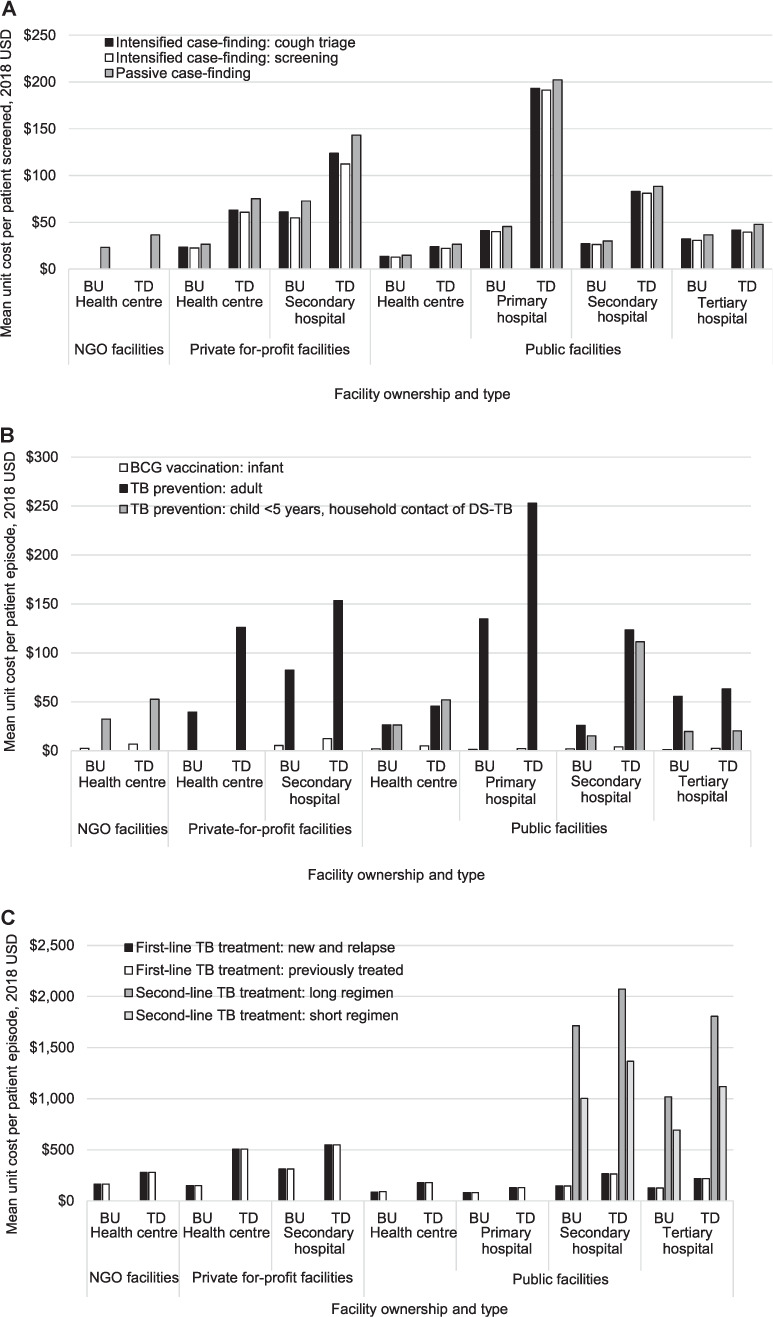
BACKGROUND: The Ethiopian Government has identified efficiency of TB services as a key priority in planning and budgeting. Understanding the magnitude and sources of inefficiencies is key to ensuring value for money and improved service provision, and a requirement from donors to justify resource needs. This study identifies the cost of providing a wide range of TB services in public and private facilities in Ethiopia.METHODS: Financial and economic unit costs were estimated from a health provider´s perspective, and collected retrospectively in 26 health facilities using both top-down (TD) and bottom-up (BU) costing approaches for each TB service output. Capacity inefficiency was assessed by investigating the variation between TD and BU unit costs where the factor was 2.0 or more.RESULTS: Overall, TD unit costs were two times higher than BU unit costs. There was some variation across facility ownership and level of care. Unit costs in urban facilities were on average 3.8 times higher than in rural facilities.CONCLUSION: We identified some substantial inefficiencies in staff, consumable and capital inputs. Addressing these inefficiencies and rearranging the TB service delivery modality would be important in ensuring the achievement of the country´s End TB strategy.
CONTEXTE: Le gouvernement éthiopien estime que l’efficacité des services antituberculeux est une priorité essentielle en matière d’organisation et de prévisions budgétaires. Il est essentiel de comprendre l’étendue et l’origine de ce qui ne fonctionne pas afin de garantir un bon rapport coût-avantages, d’améliorer la fourniture des services et de répondre aux exigences des donneurs afin de justifier les besoins en ressources. Cette étude a identifié les coûts de la fourniture d’une vaste gamme de services antituberculeux dans les établissements privés et publiques d’Éthiopie.
MÉTHODES: Les coûts unitaires financiers et économiques ont été estimés du point de vue du prestataire de services, et recueillis de manière rétrospective dans 26 centres de soins en utilisant l’approche descendante (TD) et ascendante (BU) d’évaluation des coûts pour le rendement de chaque service antituberculeux fourni. L’inefficacité des capacités a été évaluée en analysant la variation entre les coûts unitaires TD et BU associée à un facteur de 2,0 ou plus.
RÉSULTATS: Dans l’ensemble, les coûts unitaires TD étaient deux fois plus élevés que les coûts unitaires BU. Une certaine variation a été observée en fonction des propriétaires des centres et du niveau de soins. Les coûts unitaires dans les centres de soins urbains étaient en moyenne 3,8 fois plus élevés que ceux dans les centres ruraux.
CONCLUSION: Nous avons identifié d’importants points d’inefficacité au niveau du personnel, des consommables et de l’apport en capital. Il serait important de remédier à ces points d’inefficacités et de redéfinir les modalités de fourniture des soins antituberculeux afin de pouvoir satisfaire les objectifs fixés pour le pays par la stratégie de l’OMS pour mettre fin à la TB.
Conflict of interest statement
Conflicts of interest: none declared.
Figures
Similar articles
-
Cost of TB services in healthcare facilities in Kenya (No 3).Int J Tuberc Lung Dis. 2021 Dec 1;25(12):1028-1034. doi: 10.5588/ijtld.21.0129. Int J Tuberc Lung Dis. 2021. PMID: 34886934 Free PMC article.
-
Assessing the cost of providing a prevention of mother-to-child transmission of HIV/AIDS service in Ethiopia: urban-rural health facilities setting.BMC Health Serv Res. 2019 Mar 6;19(1):148. doi: 10.1186/s12913-019-3978-4. BMC Health Serv Res. 2019. PMID: 30841870 Free PMC article.
-
Recurrent costs in primary health care in Ethiopia: facility and disease specific unit costs and their components in government primary hospitals and health centers.BMC Health Serv Res. 2020 May 7;20(1):389. doi: 10.1186/s12913-020-05218-1. BMC Health Serv Res. 2020. PMID: 32381077 Free PMC article.
-
The contribution of private health facilities to the urban tuberculosis program of Afghanistan.Indian J Tuberc. 2023 Jan;70(1):8-11. doi: 10.1016/j.ijtb.2022.03.005. Epub 2022 Mar 23. Indian J Tuberc. 2023. PMID: 36740323 Review.
-
Financial burden of tuberculosis diagnosis and treatment for patients in Ethiopia: a systematic review and meta-analysis.BMC Public Health. 2024 Jan 22;24(1):260. doi: 10.1186/s12889-024-17713-9. BMC Public Health. 2024. PMID: 38254019 Free PMC article.
Cited by
-
Cost of TB services: approach and summary findings of a multi-country study (Value TB).Int J Tuberc Lung Dis. 2022 Nov 1;26(11):1006-1015. doi: 10.5588/ijtld.22.0096. Int J Tuberc Lung Dis. 2022. PMID: 36281042 Free PMC article.
References
-
- Federal Ministry of Health Addis Ababa, Ethiopia: Federal Democratic Republic of Ethiopia Ministry of Health; 2013. Guidelines for clinical and programmatic management of TB, TB/HIV and leprosy in Ethiopia.
-
- Federal Ministry of Health Addis Ababa, Ethiopia: Federal Ministry of Health; 2013. Revised strategic plan: tuberculosis, TB/HIV, MDR-TB, and leprosy prevention and control 2006–2013 EC (2013/2014–2020)
-
- Federal Ministry of Health Addis Ababa, Ethiopia: Federal Democratic Republic of Ethiopia Ministry of Health; 2015. Health Sector Transformation Plan 2015/16–2019/20 (2008–2012 EFY)
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
