

Hand grip strength-based cachexia index as a predictor of cancer cachexia and prognosis in patients with cancer
- PMID: 36447437
- PMCID: PMC9891920
- DOI: 10.1002/jcsm.13139
Hand grip strength-based cachexia index as a predictor of cancer cachexia and prognosis in patients with cancer
Abstract
Background: The cachexia index is a useful predictor for cancer cachexia and prognostic assessment. However, its use is limited because of high testing costs and complicated testing procedures. Thus, in this study, we aimed to develop a hand grip strength (HGS)-based cancer cachexia index (H-CXI) as a potential predictor of cancer cachexia and prognosis in patients with cancer.
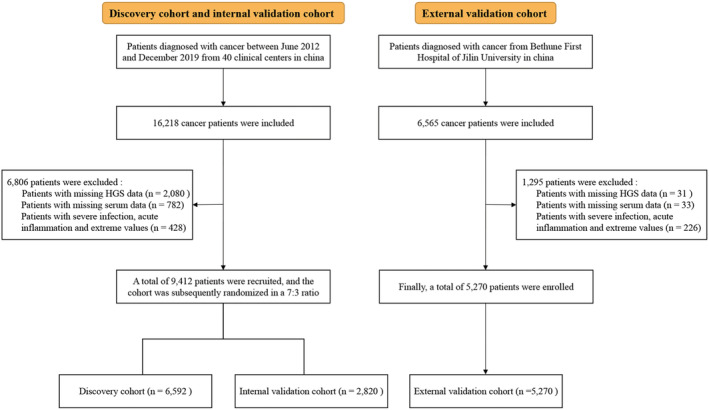
Methods: Here, 14 682 patients with cancer were studied, including the discovery (6592), internal validation (2820) and external validation (5270) cohorts. The H-CXI was calculated as [HGS (kg)/height (m)2 × serum albumin (g/L)]/neutrophil-to-lymphocyte ratio. The Kaplan-Meier method was used to create survival curves, and the log-rank test was used to compare time-event relationships between groups. A Cox proportional hazard regression model was used to determine independent risk factors for overall survival (OS). Logistic regression analysis was used to assess the association of the H-CXI with short-term outcomes and cancer cachexia.
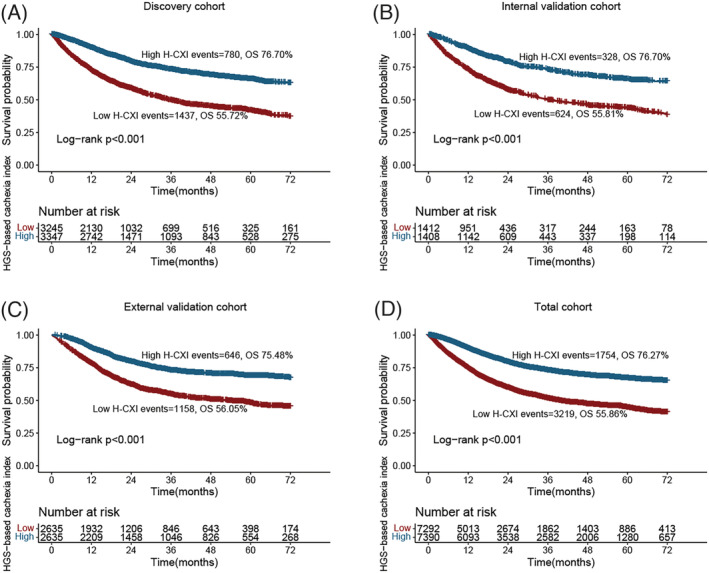
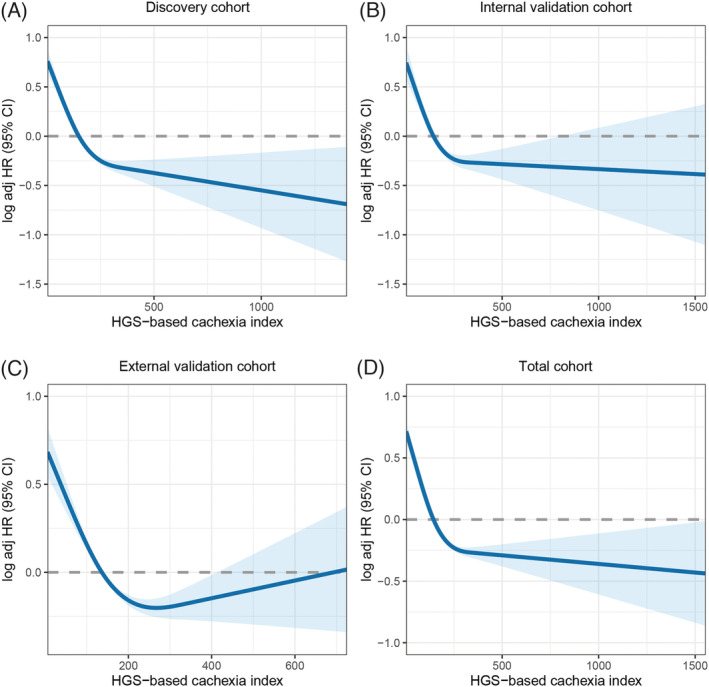
Results: There was a significant non-linear relationship between the H-CXI and OS in all cohorts. Patients with a low H-CXI had significantly lower OS than those with a high H-CXI in the discovery cohort (6-year survival percentage: 55.72% vs. 76.70%, log-rank P < 0.001), internal validation cohort (6-year survival percentage: 55.81% vs. 76.70%, log-rank P < 0.001), external validation cohort (6-year survival percentage: 56.05% vs. 75.48%, log-rank P < 0.001) and total cohort (6-year survival percentage: 55.86% vs. 76.27%, log-rank P < 0.001). Notably, the prognostic stratification effect of the H-CXI in patients with advanced-stage disease was more significant than that in patients with early-stage disease. The multivariate Cox proportional risk regression model confirmed that a low H-CXI negatively affected the prognosis of patients with cancer in the discovery cohort [hazard ratio (HR) 0.75, 95% confidence interval (CI) 0.71-0.80, P < 0.001], internal validation cohort (HR 0.79, 95 %CI 0.72-0.86, P < 0.001), external validation cohort (HR 0.84, 95% CI 0.79-0.89, P < 0.001) and total cohort (HR 0.80, 95% CI 0.77-0.83, P < 0.001). Multivariate logistic regression models showed that a low H-CXI was an independent risk factor predicting adverse short-term outcomes and cancer cachexia in patients with cancer.
Conclusions: The simple and practical H-CXI is a promising predictor for cancer cachexia and prognosis in patients with cancer.
Keywords: HGS-based cachexia index; cachexia; cancer; prognosis.
© 2022 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Kocarnik JM, Compton K, Dean FE, Fu W, Gaw BL, Harvey JD, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability‐adjusted life years for 29 cancer groups from 2010 to 2019: A systematic analysis for the global burden of disease study 2019. JAMAOncologia 2021;8:420–444. - PMC - PubMed
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249. - PubMed
-
- Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, Pletcher MA, Smith AE, Tang K, Yuan CW, Brown JC, Friedman J, He J, Heuton KR, Holmberg M, Patel DJ, Reidy P, Carter A, Cercy K, Chapin A, Douwes‐Schultz D, Frank T, Goettsch F, Liu PY, Nandakumar V, Reitsma MB, Reuter V, Sadat N, Sorensen RJD, Srinivasan V, Updike RL, York H, Lopez AD, Lozano R, Lim SS, Mokdad AH, Vollset SE, Murray CJL. Forecasting life expectancy, years of life lost, and all‐cause and cause‐specific mortality for 250 causes of death: Reference and alternative scenarios for 2016‐40 for 195 countries and territories. Lancet 2018;392:2052–2090. - PMC - PubMed
-
- Bray F, Jemal A, Grey N, Ferlay J, Forman D. Global cancer transitions according to the human development index (2008‐2030): A population‐based study. Lancet Oncol 2012;13:790–801. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
