

The BCL-2 Inhibitor Venetoclax Augments Immune Effector Function Mediated by Fas Ligand, TRAIL, and Perforin/Granzyme B, Resulting in Reduced Plasma Viremia and Decreased HIV Reservoir Size during Acute HIV Infection in a Humanized Mouse Model
- PMID: 36448802
- PMCID: PMC9769373
- DOI: 10.1128/jvi.01730-22
The BCL-2 Inhibitor Venetoclax Augments Immune Effector Function Mediated by Fas Ligand, TRAIL, and Perforin/Granzyme B, Resulting in Reduced Plasma Viremia and Decreased HIV Reservoir Size during Acute HIV Infection in a Humanized Mouse Model
Abstract
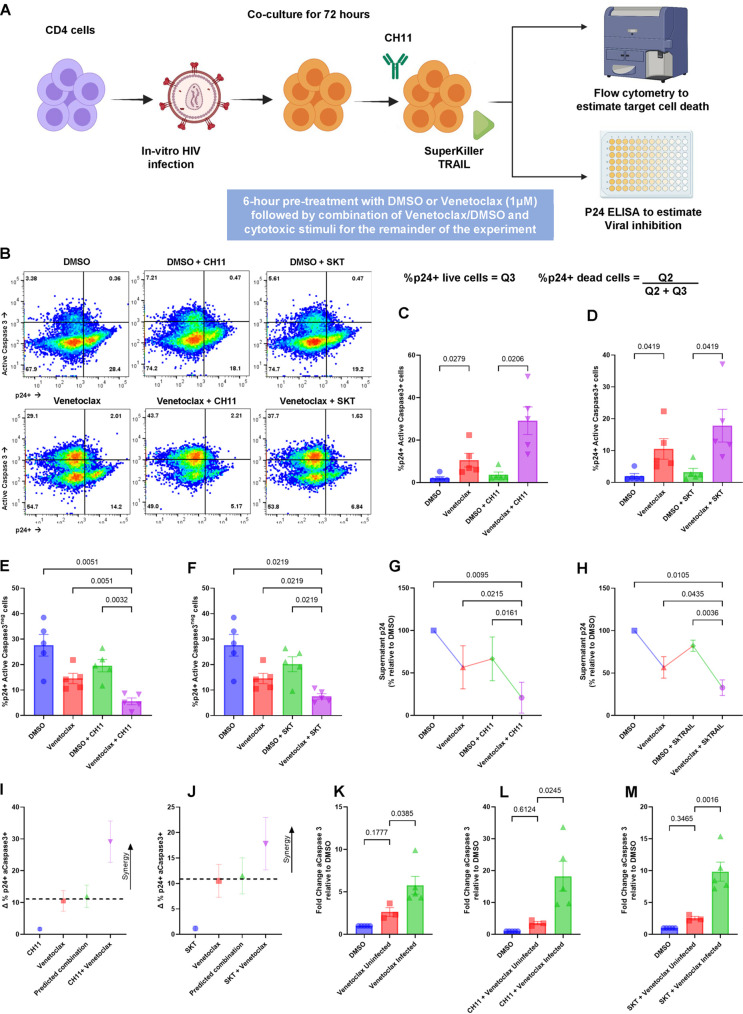
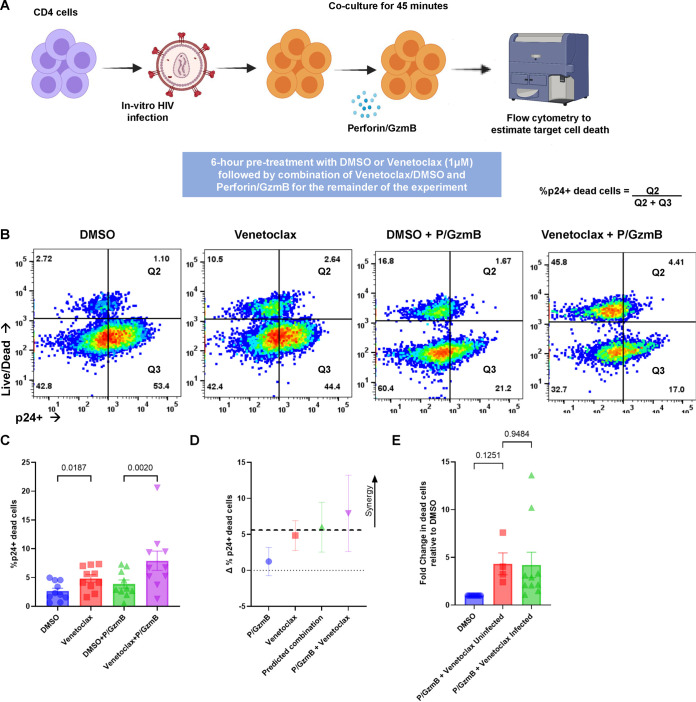
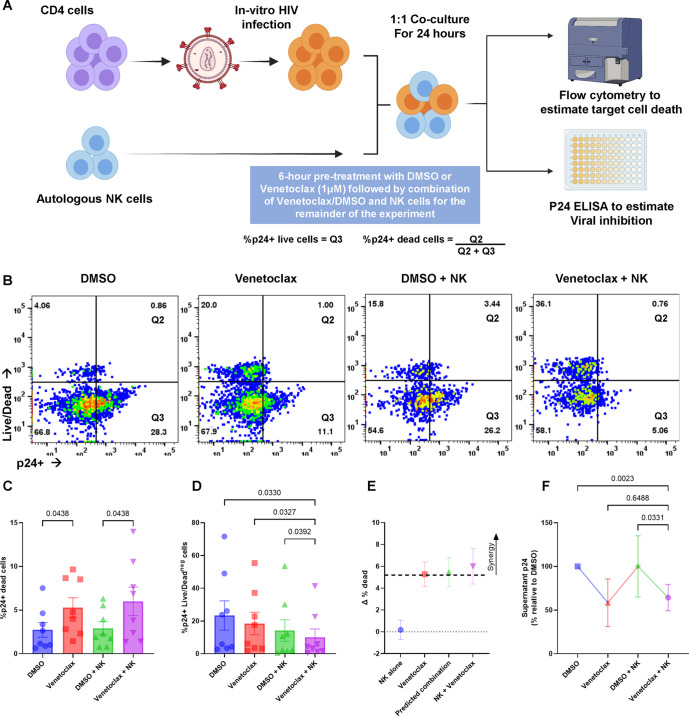
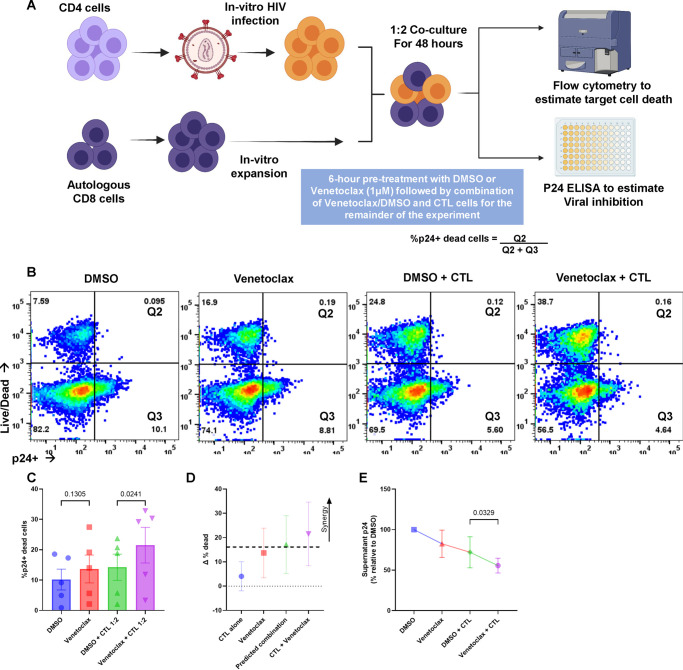
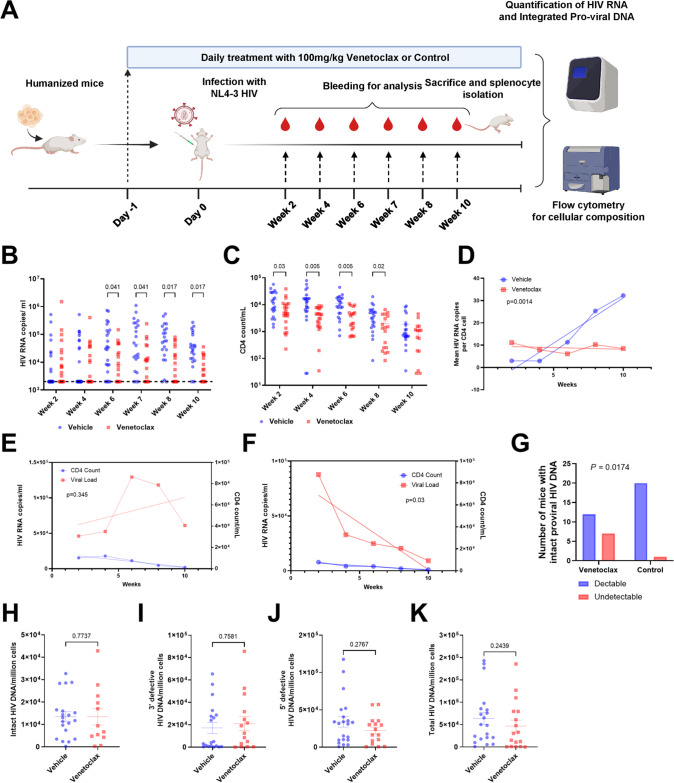
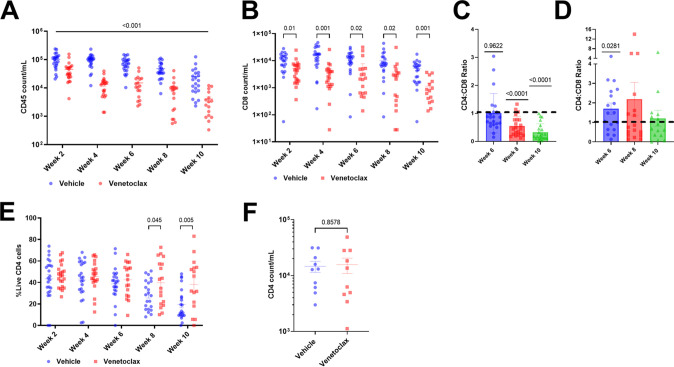
The BCL-2 prosurvival protein is implicated in HIV persistence and is a potential therapeutic target for HIV eradication efforts. We now know that cells harboring HIV are preferentially enriched for high BCL-2 expression, enabling their survival, and that the BCL-2 inhibitor venetoclax promotes the death of actively replicating HIV-infected cells in vitro and ex vivo. Herein, we assess the effect of venetoclax on immune clearance of infected cells and show that BCL-2 inhibition significantly enhances target cell killing induced by Fas ligand, TRAIL (tumor necrosis factor-related apoptosis-inducing ligand), and perforin/granzyme B and synergistically enhances autologous NK (natural killer) and CD8 cells' killing of target cells. In a humanized mouse model of acute HIV infection, venetoclax monotherapy significantly decreases plasma viremia and normalizes CD4:CD8 ratios, and results in more mice with undetectable provirus levels than control. In this model, treatment was associated with leukopenia, as has been described clinically in patients receiving venetoclax for other indications. These data confirm meaningful anti-HIV effects of venetoclax during HIV infection but suggest that venetoclax use should be combined with ART (antiretroviral therapy) to reduce toxicity. IMPORTANCE This study is the first to examine the applicability of BCL-2 inhibition in the setting of active HIV infection in vivo. Furthermore, this study demonstrates that venetoclax significantly enhances target cell killing induced by Fas ligand, TRAIL, and perforin/granzyme B and synergistically enhances autologous NK and CD8 cells' killing of target cells.
Keywords: BCL-2 family; human immunodeficiency virus; venetoclax.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Apoptosis in acute shigellosis is associated with increased production of Fas/Fas ligand, perforin, caspase-1, and caspase-3 but reduced production of Bcl-2 and interleukin-2.Infect Immun. 2002 Jun;70(6):3199-207. doi: 10.1128/IAI.70.6.3199-3207.2002. Infect Immun. 2002. PMID: 12011015 Free PMC article.
-
Natural Killer Cell Group 7 Sequence in Cytotoxic Cells Optimizes Exocytosis of Lytic Granules Essential for the Perforin-Dependent, but Not Fas Ligand-Dependent, Cytolytic Pathway.Immunohorizons. 2021 Apr 28;5(4):234-245. doi: 10.4049/immunohorizons.2100029. Immunohorizons. 2021. PMID: 33911019
-
Critical role for perforin-, Fas/FasL-, and TNFR1-mediated cytotoxic pathways in down-regulation of antigen-specific T cells during persistent viral infection.J Virol. 2002 Jan;76(2):829-40. doi: 10.1128/jvi.76.2.829-840.2002. J Virol. 2002. PMID: 11752172 Free PMC article.
-
Repurposing BCL-2 and Jak 1/2 inhibitors: Cure and treatment of HIV-1 and other viral infections.Front Immunol. 2022 Dec 9;13:1033672. doi: 10.3389/fimmu.2022.1033672. eCollection 2022. Front Immunol. 2022. PMID: 36569952 Free PMC article. Review.
-
New mechanism of organophosphorus pesticide-induced immunotoxicity.J Nippon Med Sch. 2007 Apr;74(2):92-105. doi: 10.1272/jnms.74.92. J Nippon Med Sch. 2007. PMID: 17507786 Review.
Cited by
-
The Proviral Reservoirs of Human Immunodeficiency Virus (HIV) Infection.Pathogens. 2024 Dec 30;14(1):15. doi: 10.3390/pathogens14010015. Pathogens. 2024. PMID: 39860976 Free PMC article. Review.
-
Combined dendritic cell and anti-TIGIT immunotherapy potentiates adaptive NK cells against HIV-1.EMBO Mol Med. 2025 Jul;17(7):1756-1793. doi: 10.1038/s44321-025-00255-x. Epub 2025 Jun 5. EMBO Mol Med. 2025. PMID: 40473838 Free PMC article.
-
BCL-2 Inhibition via Venetoclax at ART Initiation Induces Long-Term Reduction of the Intact SIV Reservoir.Res Sq [Preprint]. 2025 Jul 14:rs.3.rs-7060088. doi: 10.21203/rs.3.rs-7060088/v1. Res Sq. 2025. PMID: 40709247 Free PMC article. Preprint.
-
Immune-mediated strategies to solving the HIV reservoir problem.Nat Rev Immunol. 2025 Jul;25(7):542-553. doi: 10.1038/s41577-025-01136-7. Epub 2025 Feb 13. Nat Rev Immunol. 2025. PMID: 39948261 Review.
-
Venetoclax, alone and in combination with the BH3 mimetic S63845, depletes HIV-1 latently infected cells and delays rebound in humanized mice.Cell Rep Med. 2023 Sep 19;4(9):101178. doi: 10.1016/j.xcrm.2023.101178. Epub 2023 Aug 30. Cell Rep Med. 2023. PMID: 37652018 Free PMC article.
References
-
- Ananworanich J, Chomont N, Eller LA, Kroon E, Tovanabutra S, Bose M, Nau M, Fletcher JLK, Tipsuk S, Vandergeeten C, O'Connell RJ, Pinyakorn S, Michael N, Phanuphak N, Robb ML, RV217 and RV254/SEARCH010 study groups . 2016. HIV DNA set point is rapidly established in acute HIV infection and dramatically reduced by early ART. EBioMedicine 11:68–72. 10.1016/j.ebiom.2016.07.024. - DOI - PMC - PubMed
-
- Nguyen S, Deleage C, Darko S, Ransier A, Truong DP, Agarwal D, Japp AS, Wu VH, Kuri-Cervantes L, Abdel-Mohsen M, Del Rio Estrada PM, Ablanedo-Terrazas Y, Gostick E, Hoxie JA, Zhang NR, Naji A, Reyes-Terán G, Estes JD, Price DA, Douek DC, Deeks SG, Buggert M, Betts MR. 2019. Elite control of HIV is associated with distinct functional and transcriptional signatures in lymphoid tissue CD8+ T cells. Sci Transl Med 11:eaax4077. 10.1126/scitranslmed.aax4077. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
