

Association of Patient-Level and Hospital-Level Factors With Timely Fracture Care by Race
- PMID: 36449289
- PMCID: PMC9713603
- DOI: 10.1001/jamanetworkopen.2022.44357
Association of Patient-Level and Hospital-Level Factors With Timely Fracture Care by Race
Abstract
Importance: Racial disparities in treatment benchmarks have been documented among older patients with hip fractures. However, these studies were limited to patient-level evaluations.
Objective: To assess whether disparities in meeting fracture care time-to-surgery benchmarks exist at the patient level or at the hospital or institutional level using high-quality multicenter prospectively collected data; the study hypothesis was that disparities at the hospital-level reflecting structural health systems issues would be detected.
Design, setting, and participants: This cohort study was a secondary analysis of prospectively collected data in the PREP-IT (Program of Randomized trials to Evaluate Preoperative antiseptic skin solutions in orthopaedic Trauma) program from 23 sites throughout North America. The PREP-IT trials enrolled patients from 2018 to 2021, and patients were followed for 1-year. All patients with hip and femur fractures enrolled in the PREP-IT program were included in analysis. Data were analyzed April to September 2022.
Exposures: Patient-level and hospital-level race, ethnicity, and insurance status.
Main outcomes and measures: Primary outcome measure was time to surgery based on 24-hour time-to-surgery benchmarks. Multilevel multivariate regression models were used to evaluate the association of race, ethnicity, and insurance status with time to surgery. The reported odds ratios (ORs) were per 10% change in insurance coverage or racial composition at the hospital level.
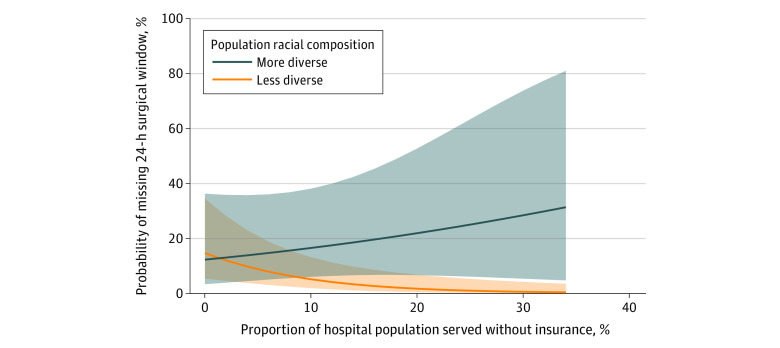
Results: A total of 2565 patients with a mean (SD) age of 64.5 (20.4) years (1129 [44.0%] men; mean [SD] body mass index, 27.3 [14.9]; 83 [3.2%] Asian, 343 [13.4%] Black, 2112 [82.3%] White, 28 [1.1%] other) were included in analysis. Of these patients, 834 (32.5%) were employed and 2367 (92.2%) had insurance; 1015 (39.6%) had sustained a femur fracture, with a mean (SD) injury severity score of 10.4 (5.8). Five hundred ninety-six patients (23.2%) did not meet the 24-hour time-to-operating-room benchmark. After controlling for patient-level characteristics, there was an independent association between missing the 24-hour benchmark and hospital population insurance coverage (OR, 0.94; 95% CI, 0.89-0.98; P = .005) and the interaction term between hospital population insurance coverage and racial composition (OR, 1.03; 95% CI, 1.01-1.05; P = .03). There was no association between patient race and delay beyond 24-hour benchmarks (OR, 0.96; 95% CI, 0.72-1.29; P = .79).
Conclusions and relevance: In this cohort study, patients who sought care from an institution with a greater proportion of patients with racial or ethnic minority status or who were uninsured were more likely to experience delays greater than the 24-hour benchmarks regardless of the individual patient race; institutions that treat a less diverse patient population appeared to be more resilient to the mix of insurance status in their patient population and were more likely to meet time-to-surgery benchmarks, regardless of patient insurance status or population-based insurance mix. While it is unsurprising that increased delays were associated with underfunded institutions, the association between institutional-level racial disparity and surgical delays implies structural health systems bias.
Conflict of interest statement
Figures
References
-
- Zweifler RM, McClure LA, Howard VJ, et al. . Racial and geographic differences in prevalence, awareness, treatment and control of dyslipidemia: the reasons for geographic and racial differences in stroke (REGARDS) study. Neuroepidemiology. 2011;37(1):39-44. doi:10.1159/000328258 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
