

Oxygen administration during surgery and postoperative organ injury: observational cohort study
- PMID: 36450405
- PMCID: PMC9710248
- DOI: 10.1136/bmj-2022-070941
Oxygen administration during surgery and postoperative organ injury: observational cohort study
Abstract
Objective: To examine whether supraphysiological oxygen administration during surgery is associated with lower or higher postoperative kidney, heart, and lung injury.
Design: Observational cohort study.
Setting: 42 medical centers across the United States participating in the Multicenter Perioperative Outcomes Group data registry.
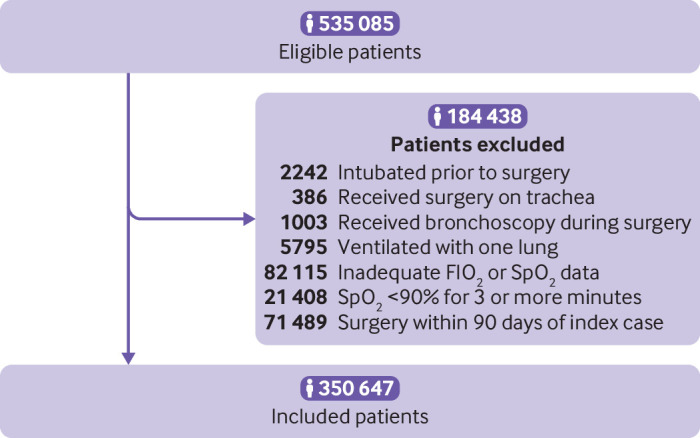
Participants: Adult patients undergoing surgical procedures ≥120 minutes' duration with general anesthesia and endotracheal intubation who were admitted to hospital after surgery between January 2016 and November 2018.
Intervention: Supraphysiological oxygen administration, defined as the area under the curve of the fraction of inspired oxygen above air (21%) during minutes when the hemoglobin oxygen saturation was greater than 92%.
Main outcomes: Primary endpoints were acute kidney injury defined using Kidney Disease Improving Global Outcomes criteria, myocardial injury defined as serum troponin >0.04 ng/mL within 72 hours of surgery, and lung injury defined using international classification of diseases hospital discharge diagnosis codes.
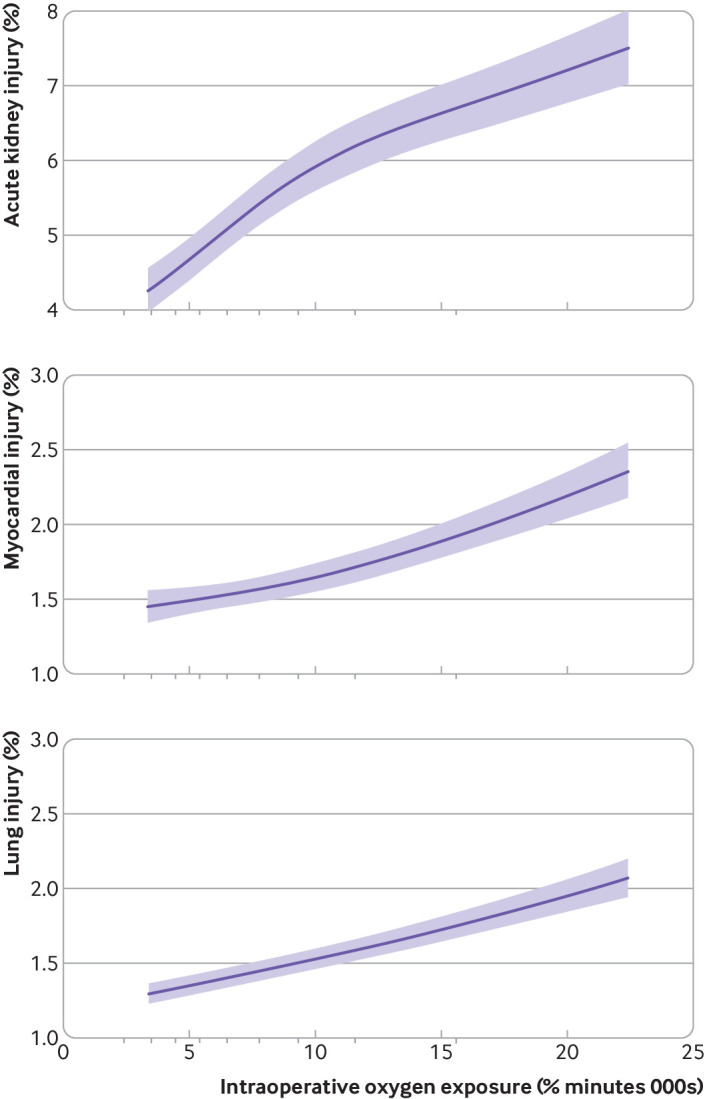
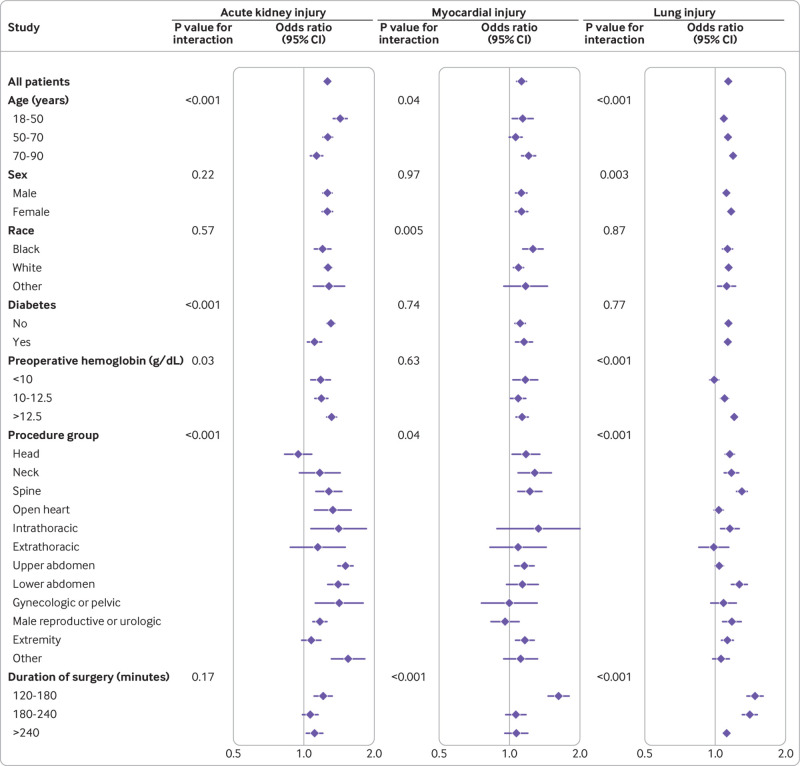
Results: The cohort comprised 350 647 patients with median age 59 years (interquartile range 46-69 years), 180 546 women (51.5%), and median duration of surgery 205 minutes (interquartile range 158-279 minutes). Acute kidney injury was diagnosed in 19 207 of 297 554 patients (6.5%), myocardial injury in 8972 of 320 527 (2.8%), and lung injury in 13 789 of 312 161 (4.4%). The median fraction of inspired oxygen was 54.0% (interquartile range 47.5%-60.0%), and the area under the curve of supraphysiological inspired oxygen was 7951% min (5870-11 107% min), equivalent to an 80% fraction of inspired oxygen throughout a 135 minute procedure, for example. After accounting for baseline covariates and other potential confounding variables, increased oxygen exposure was associated with a higher risk of acute kidney injury, myocardial injury, and lung injury. Patients at the 75th centile for the area under the curve of the fraction of inspired oxygen had 26% greater odds of acute kidney injury (95% confidence interval 22% to 30%), 12% greater odds of myocardial injury (7% to 17%), and 14% greater odds of lung injury (12% to 16%) compared with patients at the 25th centile. Sensitivity analyses evaluating alternative definitions of the exposure, restricting the cohort, and conducting an instrumental variable analysis confirmed these observations.
Conclusions: Increased supraphysiological oxygen administration during surgery was associated with a higher incidence of kidney, myocardial, and lung injury. Residual confounding of these associations cannot be excluded.
Trial registration: Open Science Framework osf.io/cfd2m.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from United States NIH, Association of University Anesthesiologists, departmental and institutional resources at each contributing medical center, Blue Cross Blue Shield of Michigan/Blue Care Network for the submitted work; DRM is chair of the data safety and monitoring board for the HOT-ROX trial (ACTRN12619000115134), an investigator initiated, multicenter international, randomized controlled trial of restrictive FIO2, liberal FIO2, and usual FIO2 in surgical patients; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Allegranzi B, Zayed B, Bischoff P, et al. WHO Guidelines Development Group . New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis 2016;16:e288-303. 10.1016/S1473-3099(16)30402-9 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources