

Surgical Treatment is Still Recommended for Patients Over 75 Years with IA NSCLC: A Predictive Model Based on Surveillance, Epidemiology and End Results Database
- PMID: 36450593
- PMCID: PMC9720806
- DOI: 10.1177/10732748221142750
Surgical Treatment is Still Recommended for Patients Over 75 Years with IA NSCLC: A Predictive Model Based on Surveillance, Epidemiology and End Results Database
Abstract
Background: To determine the populations who suitable for surgical treatment in elderly patients (age ≥ 75 y) with IA stage.
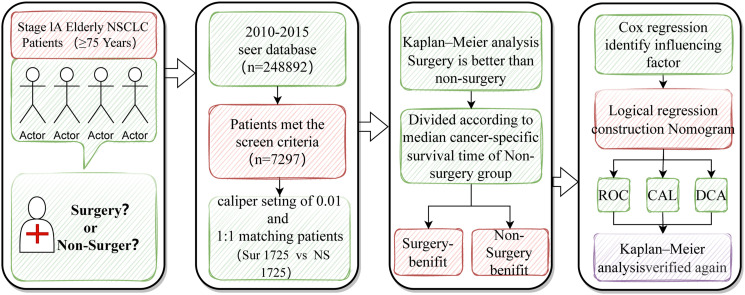
Methods: The clinical data of NSCLC patients diagnosed from 2010 to 2015 were collected from the SEER database and divided into surgery group (SG) and no-surgery groups (NSG). The confounders were balanced and differences in survival were compared between groups using PSM (Propensity score matching, PSM). Cox regression analysis was used to screen the independent factors that affect the Cancer-specific survival (CSS). The surgery group was defined as the patients who surgery-benefit and surgery-no benefit according to the median CSS of the no-surgery group, and then randomly divided into training and validation groups. A surgical benefit prediction model was constructed in the training and validation group. Finally, the model is evaluated using a variety of methods.
Results: A total of 7297 patients were included. Before PSM (SG: n = 3630; NSG: n = 3665) and after PSM (SG: n = 1725, NSG: n = 1725) confirmed that the CSS of the surgery group was longer than the no-surgery group (before PSM: 82 vs. 31 months, P < .0001; after PSM: 55 vs. 39 months, P < .0001). Independent prognostic factors included age, gender, race, marrital, tumor grade, histology, and surgery. In the surgery cohort after PSM, 1005 patients (58.27%) who survived for more than 39 months were defined as surgery beneficiaries, and the 720 patients (41.73%) were defined surgery-no beneficiaries. The surgery group was divided into training group 1207 (70%) and validation group 518 (30%). Independent prognostic factors were used to construct a prediction model. In training group (AUC = .678) and validation group (AUC = .622). Calibration curve and decision curve prove that the model has better performance.
Conclusions: This predictive model can well identify elderly patients with stage IA NSCLC who would benefit from surgery, thus providing a basis for clinical treatment decisions.
Keywords: Non-small cell lung cancer; SEER database; nomogram; predictive model; surgery.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures






References
-
- Shimoyama R, Tsutani Y, Wakabayashi M, et al. A multi-institutional randomized phase III trial comparing anatomical segmentectomy and wedge resection for clinical stage IA non-small cell lung cancer in high-risk operable patients: Japan Clinical Oncology Group Study JCOG1909 (ANSWER study). Jpn J Clin Oncol, 2020,50(10):1209-1213. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
