

Asymptomatic and symptomatic deep venous thrombosis in hospitalized acutely ill medical patients: risk factors and therapeutic implications
- PMID: 36451162
- PMCID: PMC9709753
- DOI: 10.1186/s12959-022-00433-8
Asymptomatic and symptomatic deep venous thrombosis in hospitalized acutely ill medical patients: risk factors and therapeutic implications
Abstract
Background: Acutely ill medical patients experience deep venous thrombosis (DVT) during the hospitalization, however the time course of DVT is still unclear.
Objectives: To evaluate risk factors in acutely ill hospitalized medical patients for proximal asymptomatic DVT (ADVT) and symptomatic DVT (SDVT) at admission and discharge.
Patients/methods: In this prospective observational study, consecutive acutely ill medical patients (hospitalized mainly for acute medical disease as infections, neoplasm, anemia, heart failure) underwent compression ultrasonography (CUS) of proximal lower limb veins within 48 h from admission and at discharge to diagnose ADVT and SDVT. Covid-19 patients, anticoagulant therapy, surgical procedures, acute SDVT, and acute pulmonary embolism, were exclusion criteria. Biographical characteristics at hospitalization, D-Dimer (assessed by ELISA)) and DD-improve score.
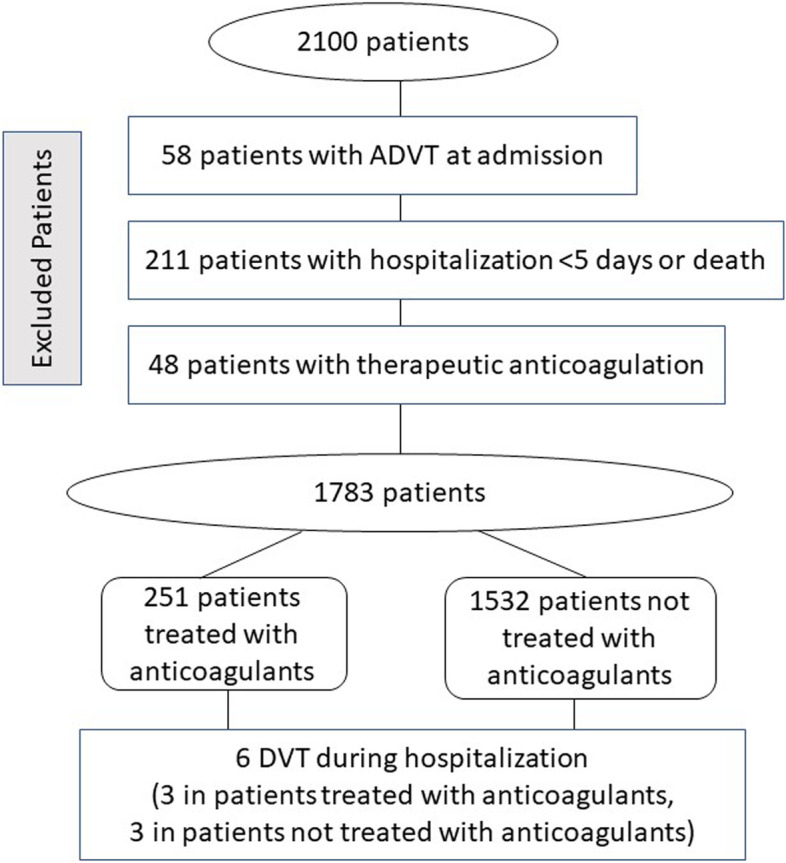
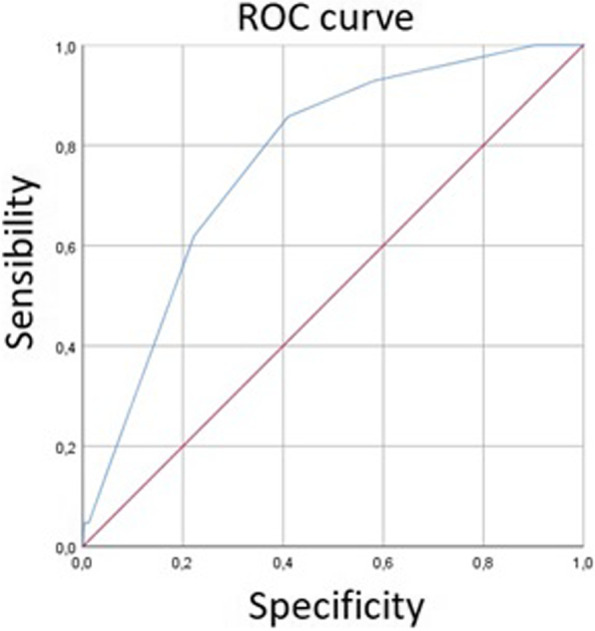
Results: Of 2,100 patients (1002 females, 998 males, age 71 ± 16 years) 58 (2.7%) had proximal ADVT at admission. Logistic regression analysis showed that age, and active cancer were independently associated with ADVT at admission. The median length of hospitalization was 10 days [interquartile range: 6-15]. During the hospital stay, 6 patients (0.3%) with a negative CUS at admission experienced DVT (2 SDVT and 4 ADVT). In the subgroup of patients (n = 1118), in whom D-dimer was measured at admission, D-Dimer and IMPROVE-DD score were associated with ADVT at admission (n = 37) and with all DVT (n = 42) at discharge. ROC curve defined an IMPROVE-DD score of 2.5 as the optimal cut-off for discriminating patients with and without thrombotic events.
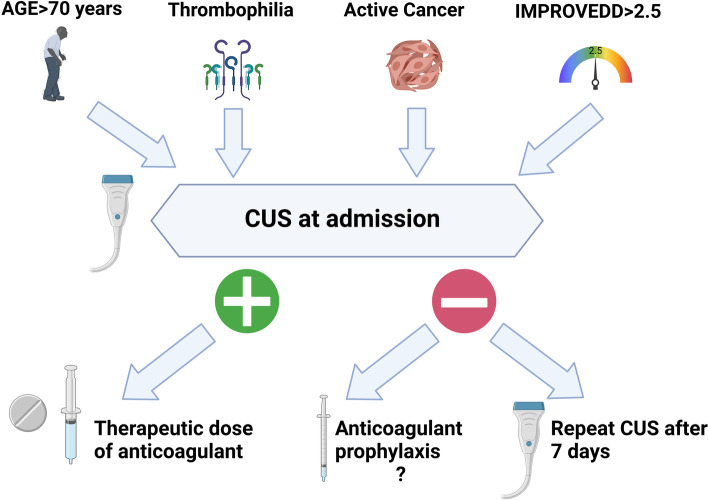
Conclusions: We provide evidence of early development of ADVT in unselected acutely ill medical patients suggesting the need of investigating patients by CUS immediately after hospital admission (within 48 h). Advanced age, active cancer, known thrombophilia and increased IMPROVE-DD score may identify patients at risk. The benefit of anticoagulation needs to be investigated in patients with these specific risk factors and negative CUS at admission.
Trial registration: NCT03157843.
Keywords: Anticoagulants; Asymptomatic deep venous thrombosis; Compression ultrasound; Deep venous thrombosis; Medical patient.
© 2022. The Author(s).
Conflict of interest statement
LL, GV, AS, CG, RDG, SB, PC, AP, FO, AP, MB, GDM, LF, CL, AS, EE, PP, MFA, JH, FV have nothing to disclose. All the authors declare that they have no conflicts of interest concerning this paper.
Figures
References
-
- Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuunemann HJ. American College of Chest Physicians Antithrombotic T, Prevention of Thrombosis P: Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:7S–47S. doi: 10.1378/chest.1412S3. - DOI - PMC - PubMed
-
- Schunemann HJ, Cushman M, Burnett AE, Kahn SR, Beyer-Westendorf J, Spencer FA, Rezende SM, Zakai NA, Bauer KA, Dentali F, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. 2018;2:3198–3225. doi: 10.1182/bloodadvances.2018022954. - DOI - PMC - PubMed
-
- Flanders SA, Greene MT, Grant P, Kaatz S, Paje D, Lee B, Barron J, Chopra V, Share D, Bernstein SJ. Hospital performance for pharmacologic venous thromboembolism prophylaxis and rate of venous thromboembolism : a cohort study. JAMA Intern Med. 2014;174:1577–1584. doi: 10.1001/jamainternmed.2014.3384. - DOI - PubMed
