

Non-REM sleep in major depressive disorder
- PMID: 36451376
- PMCID: PMC9723407
- DOI: 10.1016/j.nicl.2022.103275
Non-REM sleep in major depressive disorder
Abstract
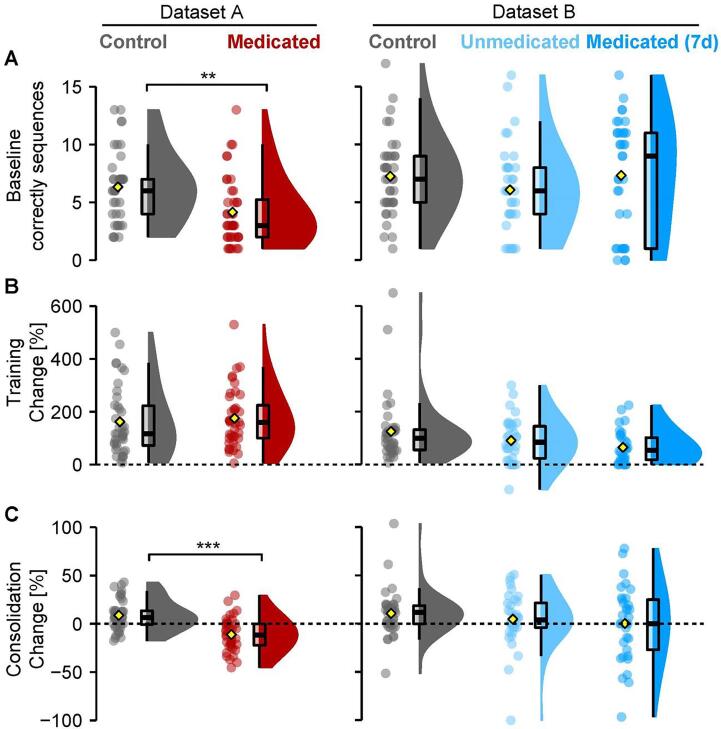
Disturbed sleep is a key symptom in major depressive disorder (MDD). REM sleep alterations are well described in the current literature, but little is known about non-REM sleep alterations. Additionally, sleep disturbances relate to a variety of cognitive symptoms in MDD, but which features of non-REM sleep EEG contribute to this, remains unknown. We comprehensively analyzed non-REM sleep EEG features in two central channels in three independently collected datasets (N = 284 recordings of 216 participants). This exploratory and descriptive study included MDD patients with a broad age range, varying duration and severity of depression, unmedicated or medicated, age- and gender-matched to healthy controls. We explored changes in sleep architecture including sleep stages and cycles, spectral power, sleep spindles, slow waves (SW), and SW-spindle coupling. Next, we analyzed the association of these sleep features with acute measures of depression severity and overnight consolidation of procedural memory. Overall, no major systematic alterations in non-REM sleep architecture were found in patients compared to controls. For the microstructure of non-REM sleep, we observed a higher spindle amplitude in unmedicated patients compared to controls, and after the start of antidepressant medication longer SWs with lower amplitude and a more dispersed SW-spindle coupling. In addition, long-term, but not short-term medication seemed to lower spindle density. Overnight procedural memory consolidation was impaired in medicated patients and associated with lower sleep spindle density. Our results suggest that alterations of non-REM sleep EEG in MDD might be more subtle than previously reported. We discuss these findings in the context of antidepressant medication intake and age.
Keywords: Antidepressant; Coupling; Depression; EEG; Medication; Non-REM sleep; Procedural memory consolidation; Sleep cycle; Sleep spindles; Slow waves.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
-
- Albouy G., King B.R., Maquet P., Doyon J. Hippocampus and striatum: Dynamics and interaction during acquisition and sleep-related motor sequence memory consolidation. Hippocampus. 2013;23:985–1004. - PubMed
-
- Allen, M., Poggiali, D., Whitaker, K., Marshall, T.R., Kievit, R., 2018. Raincloud Plots: A Multi-Platform Tool for Robust Data Visualization. PeerJ Inc; 2018. doi.org/10.7287/peerj.preprints.27137v1. - PMC - PubMed
-
- Armitage R., Hoffmann R., Trivedi M., Rush A.J. Slow-wave activity in NREM sleep: sex and age effects in depressed outpatients and healthy controls. Psychiatry Res. 1992;95:201–213. - PubMed
-
- Aust, F., Barth, M., 2018. Papaja: Prepare Reproducible APA Journal Articles with R Markdown. 2018; Retrieved from https://github.com/crsh/papaja.
-
- Benca R.M., Obermeyer W.H., Thisted R.A., Gillin J.C. Sleep and psychiatric disorders: a meta-Analysis. Arch. Gen. Psychiatry. 1992;49:651–668. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
