

Paradoxical worsening of bradycardia following atropine administration
- PMID: 36451706
- PMCID: PMC9662156
- DOI: 10.29045/14784726.2022.09.7.2.38
Paradoxical worsening of bradycardia following atropine administration
Abstract
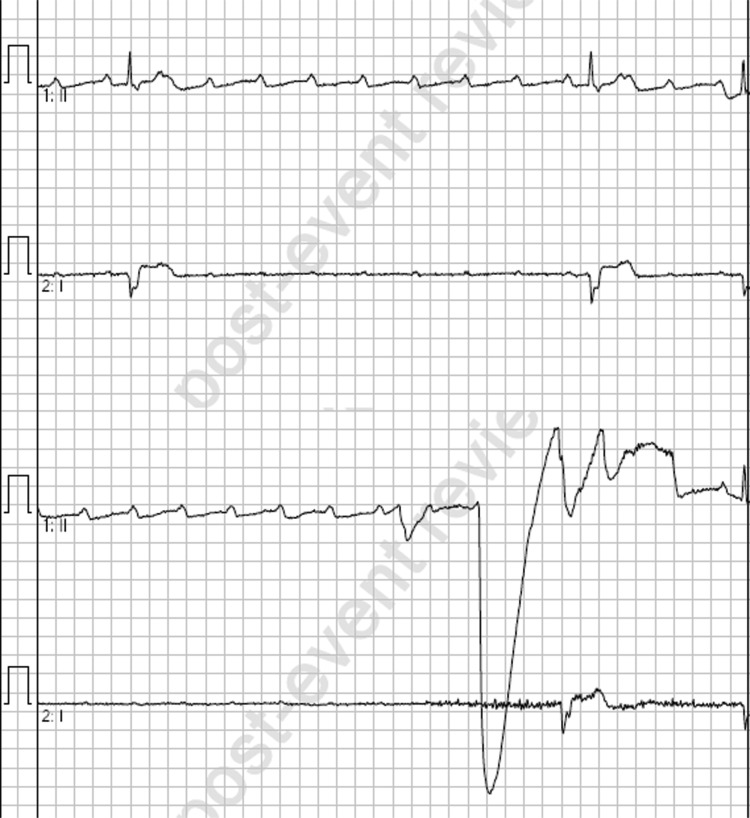
Introduction: Bradyarrhythmias are a common entity in both emergency and out-of-hospital (OOH) medicine. In unstable bradycardic patients, paramedics will often initiate life-saving therapies in the OOH setting. Clinical guidelines for bradyarrhythmias are largely consistent across the globe, with intravenous (IV) atropine recommended as a first-line therapy, escalating to IV adrenaline or isoprenaline and transcutaneous pacing where atropine is unsuccessful. In this case report, we describe a case in the OOH setting of ventricular standstill following the administration of atropine to a patient with bradycardia and 2:1 heart block.
Case presentation: The patient was a 77-year-old female presenting with a symptomatic 2:1 heart block. Following a single dose of 600 micrograms IV atropine, the patient deteriorated into ventricular standstill with a loss of consciousness and decorticate posturing. The patient was successfully managed with an IV infusion of adrenaline and subsequently received an implanted pacemaker in hospital.
Conclusion: The paradoxical worsening of this patient's bradycardia following atropine administration may have been related to the location of the heart block. It has been shown that patients with atrioventricular blocks at the level of the His-Purkinje fibres (infranodal) are at an increased risk of adverse events following atropine administration, while those at the nodal level or secondary to increased vagal tone are more likely to respond favourably. Paramedics should be prepared to manage unexpected adverse events secondary to atropine administration in patients with heart block.
Keywords: adverse event; atropine; bradycardia; paramedic.
© 2022 The Author(s).
Conflict of interest statement
None declared.
Figures



References
-
- Barold S. S. (2001). 2:1 atrioventricular block: Order from chaos. American Journal of Emergency Medicine, 19(3), 214–217. - PubMed
-
- Bernheim A., Fatio R., Kiowski W., Weilenmann D., Rickli H. & Rocca H. P. (2004). Atropine often results in complete atrioventricular block or sinus arrest after cardiac transplantation: An unpredictable and dose-independent phenomenon. Transplantation, 77(8), 1181–1185. - PubMed
-
- Beygui F., Castren M., Brunetti N. D., Rosell-Ortiz F., Christ M., Zeymer U., Huber K., Folke F., Svensson L., Bueno H., Hof A. V., Nikolaou N., Nibbe L., Charpentier S., Swahn E., Tubaro M., Goldstein P. & ACCA study group on pre-hospital care. (2020). Pre-hospital management of patients with chest pain and/or dyspnoea of cardiac origin. European Heart Journal. Acute Cardiovascular Care, 9(Suppl 1), 59–81. - PubMed
-
- Bhargava K. & India G. (2012). Atrioventricular block. Journal of Clinical and Preventative Cardiology, 1, 44–46.
LinkOut - more resources
Full Text Sources