

Case Reports
doi: 10.1016/j.case.2022.06.008.
eCollection 2022 Nov.
Stress Cardiomyopathy: The Midventricular Variant
Affiliations
- PMID: 36451868
- PMCID: PMC9703095
- DOI: 10.1016/j.case.2022.06.008
Item in Clipboard
Case Reports
Stress Cardiomyopathy: The Midventricular Variant
CASE (Phila).
.
No abstract available
Keywords: Midventricular takotsubo; Stress cardiomyopathy; Takotsubo cardiomyopathy.
Figures


Twelve-lead ECG acquired on admission (asymptomatic) demonstrates sinus bradycardia and mild nonspecific T-wave changes in leads V1-V3.
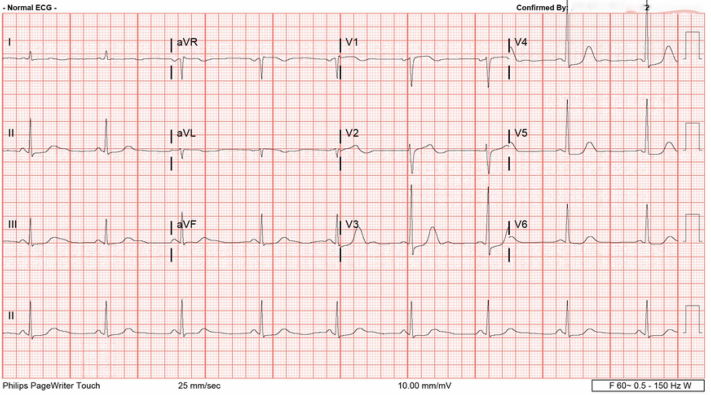
Twelve-lead ECG acquired during the episode of severe chest pain demonstrates sinus bradycardia with ST depression suggesting myocardial ischemia in leads V3-V5.

Parasternal long-axis images acquired at end diastole (left) and end systole (right) demonstrate a severe, midventricular, noncoronary pattern RWMA (arrows).

Two-dimensional TTE, apical long-axis view in diastole (left) and systole (right), demonstrates RWMAs at the midanteroseptal and inferolateral ventricular walls (arrows).
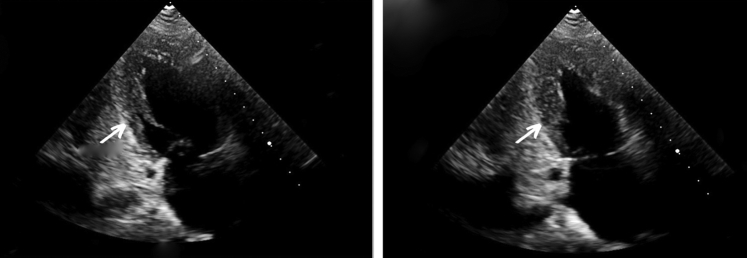
Two-dimensional TTE, apical 2-chamber view in diastole (left) and systole (right), demonstrates RWMAs at the midanterior and inferior ventricular level walls (arrows).

Two-dimensional TTE, apical 4-chamber view acquired at end diastole (left) and end systole (right), demonstrates akinesis at the midventricular myocardial wall segments (arrows).
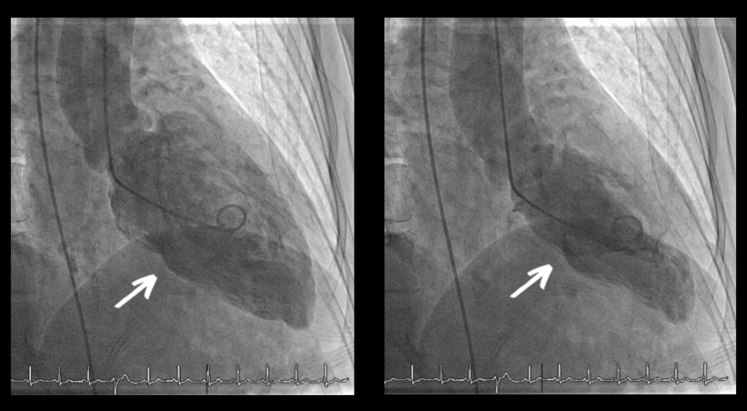
Left ventriculogram, right anterior oblique orientation in diastole (left) and systole (right), demonstrates normal apical and basal contractility with dyskinetic midventricular motion (arrows).
References
-
- Templin C., Ghadri J.R., Diekmann J., Napp L.C., Bataiosu D.R., Jaguszewski, et al. Clinical myopathy. N Engl J Med. 2015;373:929–938. - PubMed
-
- Scantlebury D.C., Prasad A. Diagnosis of Takotsubo cardiomyopathy. Circ J. 2014;78:2129–2139. - PubMed
-
- Litvinov I.V., Kotowycz M.A., Wassmann S. Iatrogenic epinephrine-induced reverse Takotsubo cardiomyopathy: direct evidence supporting the role of catecholamines in the pathophysiology of the “broken heart syndrome”. Clin Res Cardiol. 2009;98:457–462. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
