

On-treatment Comparative Effectiveness of Vitamin K Antagonists and Direct Oral Anticoagulants in GARFIELD-VTE, and Focus on Cancer and Renal Disease
- PMID: 36452204
- PMCID: PMC9633227
- DOI: 10.1055/s-0042-1757744
On-treatment Comparative Effectiveness of Vitamin K Antagonists and Direct Oral Anticoagulants in GARFIELD-VTE, and Focus on Cancer and Renal Disease
Abstract
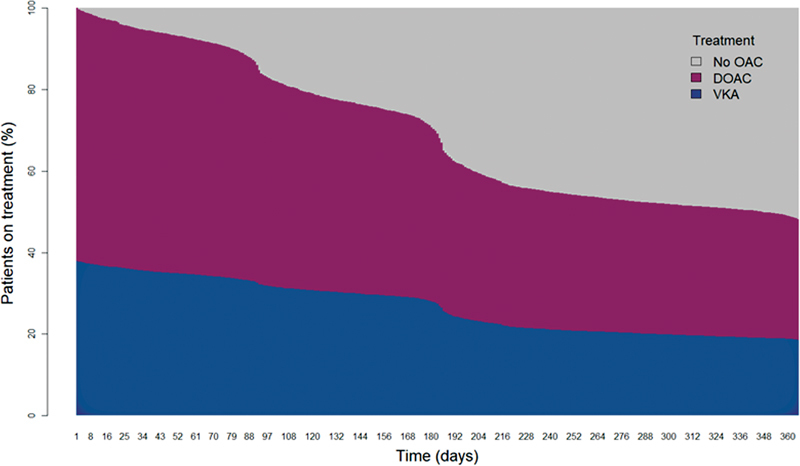
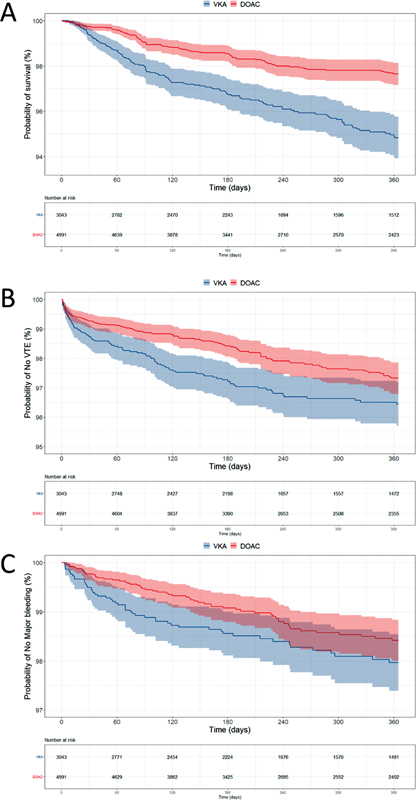
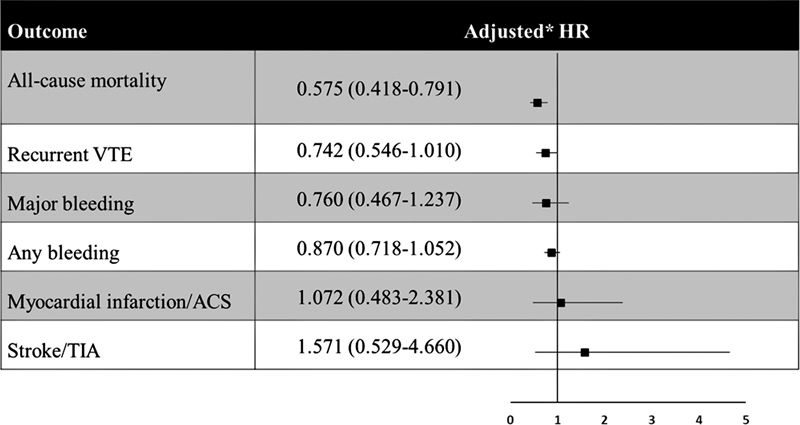
Background Direct oral anticoagulants (DOACs) provide a safe, effective alternative to vitamin K antagonists (VKAs) for venous thromboembolism (VTE) treatment, as shown via intention-to-treat comparative effectiveness analysis. However, on-treatment analysis is imperative in observational studies because anticoagulation choice and duration are at investigators' discretion. Objectives The aim of the study is to compare the effectiveness of DOACs and VKAs on 12-month outcomes in VTE patients using on-treatment analysis. Methods The Global Anticoagulant Registry in the FIELD - VTE (GARFIELD-VTE) is a world-wide, prospective, non-interventional study observing treatment of VTE in routine clinical practice. Results In total, 8,034 patients received VKAs ( n = 3,043, 37.9%) or DOACs ( n = 4,991, 62.1%). After adjustment for baseline characteristics and follow-up bleeding events, and accounting for possible time-varying confounding, all-cause mortality was significantly lower with DOACs than VKAs (hazard ratio: 0.58 [95% confidence interval 0.42-0.79]). Furthermore, patients receiving VKAs were more likely to die of VTE complications (4.9 vs. 2.2%) or bleeding (4.9 vs. 0.0%). There was no significant difference in rates of recurrent VTE (hazard ratio: 0.74 [0.55-1.01]), major bleeding (hazard ratio: 0.76 [0.47-1.24]), or overall bleeding (hazard ratio: 0.87 [0.72-1.05]) with DOACs or VKAs. Unadjusted analyses suggested that VKA patients with active cancer or renal insufficiency were more likely to die than patients treated with DOAC (52.51 [37.33-73.86] vs. 26.52 [19.37-36.29] and 9.97 [7.51-13.23] vs. 4.70 [3.25-6.81] per 100 person-years, respectively). Conclusion DOACs and VKAs had similar rates of recurrent VTE and major bleeding. However, DOACs were associated with reduced all-cause mortality and a lower likelihood of death from VTE or bleeding compared with VKAs.
Keywords: anticoagulation; direct oral anticoagulants; on-treatment comparative effectiveness; venous thromboembolism; vitamin K antagonists.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. ( https://creativecommons.org/licenses/by/4.0/ ).
Conflict of interest statement
Conflict of Interest S.H. received personal fees from Bayer, BMS, Daiichi-Sankyo, Portola, Sanofi, outside the submitted work. K.P. received consultancy fees from Johnson & Johnson and Artivion, Inc. W.A. Research Grant from Bayer Pharma AG, Honoraria from Bayer Pharma AG, Bristol Myers Squibb, Pfizer, Daiichi-Sankyo, Aspen, Sanofi, Mylan, Norgine, and Leo Pharma. S.Z.G. received research grants from BiO2 Medical, Boehringer-Ingelheim, BMS, BTG EKOS, Daiichi, Janssen, NHLBI, Thrombosis Research Institute, Personal fee from Agile, Bayer, Boehringer-Ingelheim, BMS, Daiichi, Janssen, Portola, and Zafgen. S.G. received research funding from Sanofi, Pfizer, Ono, AMED (A368TS), and Bristol-Myers Squibb; consultation fee from Bristol-Myers Squibb, Jansen, and Antos. L.M. Grants and personal fees from Bayer Pharma AG, Boehringer-Ingelheim, Pfizer and Daiichi-Sankyo, and support by Italian Ministry of Health Ricerca Corrente – IRCCS MultiMedica. P.P. received personal fees from Bayer Pharma AG, Pfizer, Daiichi-Sankyo and Sanofi. S.S. received speaker fees from Bayer Pharma AG, Boehringer-Ingelheim, Bristol Meyer Squibb, Daiichi-Sankyo, Sanofi Aventis and Pfizer, consultancy fees from Bayer Pharma AG, Boehringer-Ingelheim, Daiichi-Sankyo, Sanofi Aventis, Aspen and Pfizer. A.G.G.T. received personal fees from Bayer Healthcare, Janssen Pharmaceutical Research & Development LLC, Astellas, Portola, and Takeda. J.I.W. received research support from Canadian Institutes of Health Research, Heart and Stroke Foundation, and the Canadian Fund for Innovation. Honoraria from Alnylam, Anthos, Bayer, Boehringer-Ingelheim, Bristol Myers Squibb, Daiichi-Sankyo, Ionis, Janssen, Merck, Pfizer, PhaseBio, and Servier. P.M. received Honoraria from Bayer Pharma AG and Portolo. H.t.C. received research support from Bayer; consulting fees from Pfizer, Leo, Bayer, Alexion, Alveron; stockholder Coagulation Profile. E.P. received personal fees from Sanofi, Takeda, Boehringer Ingelheim, Pfizer, Bristol-Myers Squibb, Bayer, AstraZeneca. M.C. received grants from Pfizer/BMS, Canadian Institutes of Health Research, grants and personal fees from Leo Pharma, Bayer, personal fees from Sanofi Aventis, Pfizer, Bristol Myers Squibb. C.J.S. declares personal fees from Bayer, Boehringer Ingelheim. H.G. declared personal fees from Pfizer, Bayer, Boehringer Ingelheim. A.K.K. received grants from Bayer AG and Sanofi; personal fees from Bayer AG, Janssen, Pfizer, Sanofi, Verseon, and Anthos Therapeutics. A.E.F., H.B., P.A., P.J., and G.K. declare no conflict of interest.
Figures
References
-
- Hokusai-VTE Investigators . Büller H R, Décousus H, Grosso M A. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406–1415. - PubMed
-
- RE-COVER Study Group . Schulman S, Kearon C, Kakkar A K. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–2352. - PubMed
-
- EINSTEIN Investigators . Bauersachs R, Berkowitz S D, Brenner B. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499–2510. - PubMed
-
- AMPLIFY Investigators . Agnelli G, Buller H R, Cohen A. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(09):799–808. - PubMed
-
- SOX trial investigators Kahn S R, Shapiro S, Wells P S.Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial Lancet 2014383(9920):880–888. - PubMed
LinkOut - more resources
Full Text Sources
