

Practice-oriented solutions integrating intraoperative electron irradiation and personalized proton therapy for recurrent or unresectable cancers: Proof of concept and potential for dual FLASH effect
- PMID: 36452493
- PMCID: PMC9703091
- DOI: 10.3389/fonc.2022.1037262
Practice-oriented solutions integrating intraoperative electron irradiation and personalized proton therapy for recurrent or unresectable cancers: Proof of concept and potential for dual FLASH effect
Erratum in
-
Corrigendum: Practice-oriented solutions integrating intraoperative electron irradiation and personalized proton therapy for recurrent or unresectable cancers: Proof of concept and potential for dual FLASH effect.Front Oncol. 2023 Jan 18;12:1116433. doi: 10.3389/fonc.2022.1116433. eCollection 2022. Front Oncol. 2023. PMID: 36741712 Free PMC article.
Abstract
Background: Oligo-recurrent disease has a consolidated evidence of long-term surviving patients due to the use of intense local cancer therapy. The latter combines real-time surgical exploration/resection with high-energy electron beam single dose of irradiation. This results in a very precise radiation dose deposit, which is an essential element of contemporary multidisciplinary individualized oncology.
Methods: Patient candidates to proton therapy were evaluated in Multidisciplinary Tumor Board to consider improved treatment options based on the institutional resources and expertise. Proton therapy was delivered by a synchrotron-based pencil beam scanning technology with energy levels from 70.2 to 228.7 MeV, whereas intraoperative electrons were generated in a miniaturized linear accelerator with dose rates ranging from 22 to 36 Gy/min (at Dmax) and energies from 6 to 12 MeV.
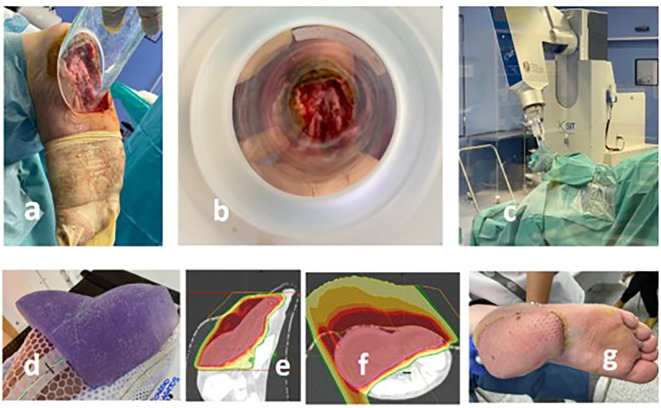
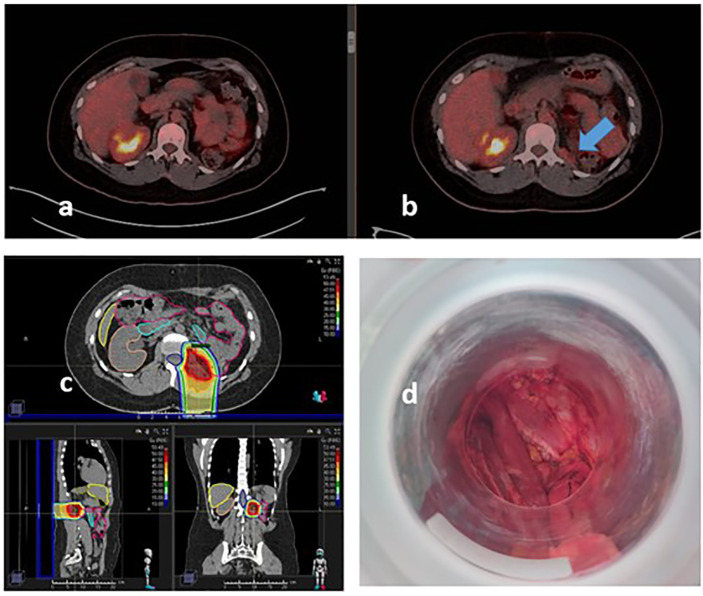
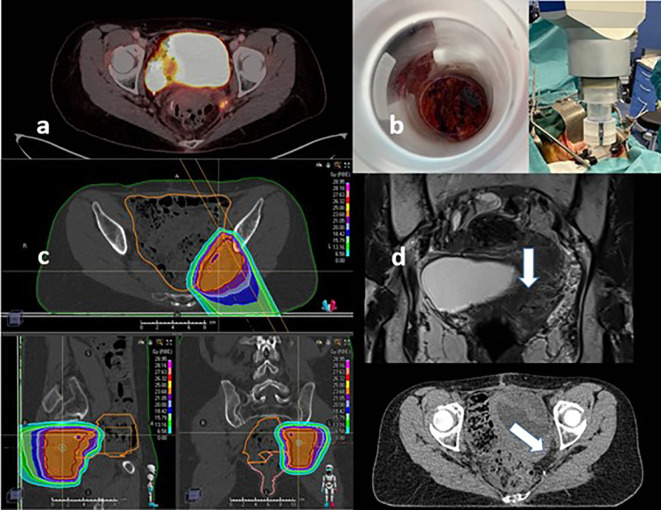
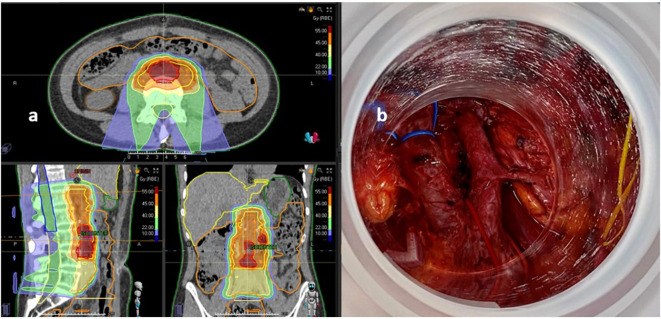
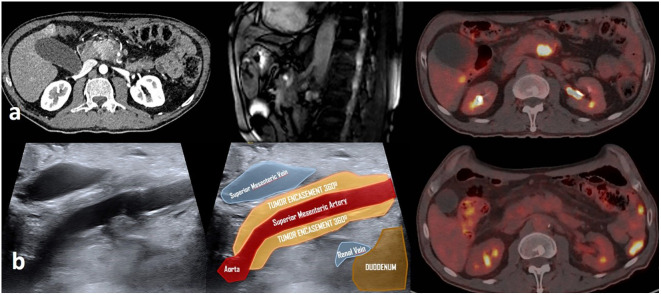
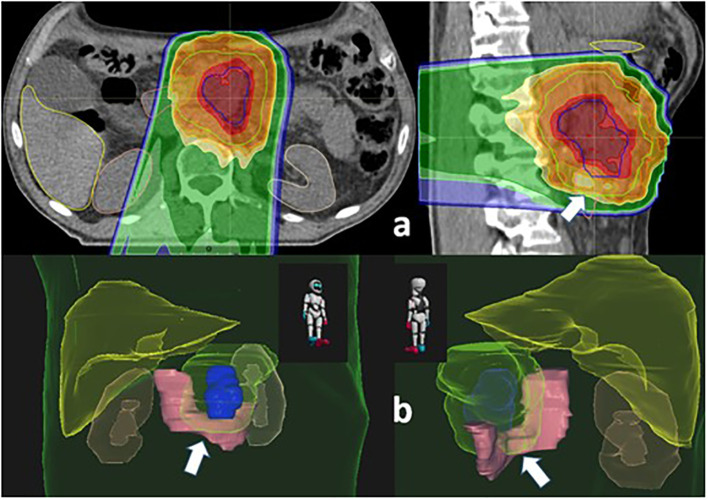
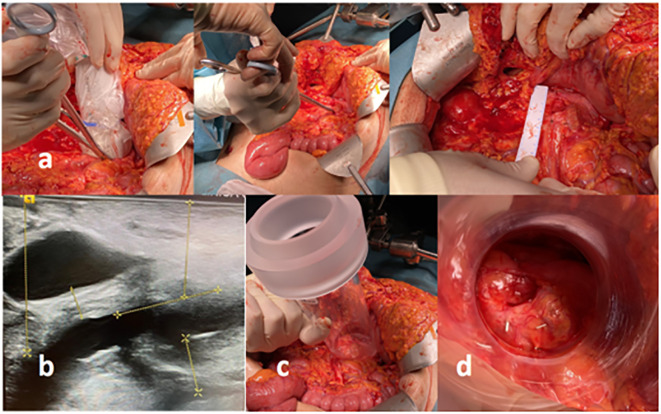
Results: In a period of 24 months, 327 patients were treated with proton therapy: 218 were adults, 97 had recurrent cancer, and 54 required re-irradiation. The specific radiation modalities selected in five cases included an integral strategy to optimize the local disease management by the combination of surgery, intraoperative electron boost, and external pencil beam proton therapy as components of the radiotherapy management. Recurrent cancer was present in four cases (cervix, sarcoma, melanoma, and rectum), and one patient had a primary unresectable locally advanced pancreatic adenocarcinoma. In re-irradiated patients (cervix and rectum), a tentative radical total dose was achieved by integrating beams of electrons (ranging from 10- to 20-Gy single dose) and protons (30 to 54-Gy Relative Biological Effectiveness (RBE), in 10-25 fractions).
Conclusions: Individual case solution strategies combining intraoperative electron radiation therapy and proton therapy for patients with oligo-recurrent or unresectable localized cancer are feasible. The potential of this combination can be clinically explored with electron and proton FLASH beams.
Keywords: cancer; electron FLASH; oligorrecurrent; proton therapy FLASH; reirradiation.
Copyright © 2022 Calvo, Ayestaran, Serrano, Cambeiro, Palma, Meiriño, Morcillo, Lapuente, Chiva, Aguilar, Azcona, Pedrero, Pascau, Delgado, Aristu and Prezado.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Corrigendum: Practice-oriented solutions integrating intraoperative electron irradiation and personalized proton therapy for recurrent or unresectable cancers: Proof of concept and potential for dual FLASH effect.Front Oncol. 2023 Jan 18;12:1116433. doi: 10.3389/fonc.2022.1116433. eCollection 2022. Front Oncol. 2023. PMID: 36741712 Free PMC article.
-
Use of single-energy proton pencil beam scanning Bragg peak for intensity-modulated proton therapy FLASH treatment planning in liver-hypofractionated radiation therapy.Med Phys. 2022 Oct;49(10):6560-6574. doi: 10.1002/mp.15894. Epub 2022 Aug 17. Med Phys. 2022. PMID: 35929404
-
Clinical feasibility of combining intraoperative electron radiation therapy with minimally invasive surgery: a potential for electron-FLASH clinical development.Clin Transl Oncol. 2023 Feb;25(2):429-439. doi: 10.1007/s12094-022-02955-z. Epub 2022 Sep 28. Clin Transl Oncol. 2023. PMID: 36169803 Free PMC article.
-
How successful is high-dose (> or = 60 Gy) reirradiation using mainly external beams in salvaging local failures of nasopharyngeal carcinoma?Int J Radiat Oncol Biol Phys. 1998 Mar 1;40(4):897-913. doi: 10.1016/s0360-3016(97)00854-7. Int J Radiat Oncol Biol Phys. 1998. PMID: 9531376 Review.
-
Intra-Operative Electron Radiation Therapy: An Update of the Evidence Collected in 40 Years to Search for Models for Electron-FLASH Studies.Cancers (Basel). 2022 Jul 29;14(15):3693. doi: 10.3390/cancers14153693. Cancers (Basel). 2022. PMID: 35954357 Free PMC article. Review.
References
-
- Prades J, Remue E, van Hoof E, Borras JM. Is it worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy (2015) 119(4):464–74. doi: 10.1016/j.healthpol.2014.09.006 - DOI - PubMed
-
- Pillay B, Wootten AC, Crowe H, Corcoran N, Tran B, Bowden P, et al. . The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat Rev (2016) 42:56–72. doi: 10.1016/j.ctrv.2015.11.007 - DOI - PubMed
LinkOut - more resources
Full Text Sources