

Trends in Cases, Hospitalizations, and Mortality Related to the Omicron BA.4/BA.5 Subvariants in South Africa
- PMID: 36453094
- PMCID: PMC10110264
- DOI: 10.1093/cid/ciac921
Trends in Cases, Hospitalizations, and Mortality Related to the Omicron BA.4/BA.5 Subvariants in South Africa
Abstract
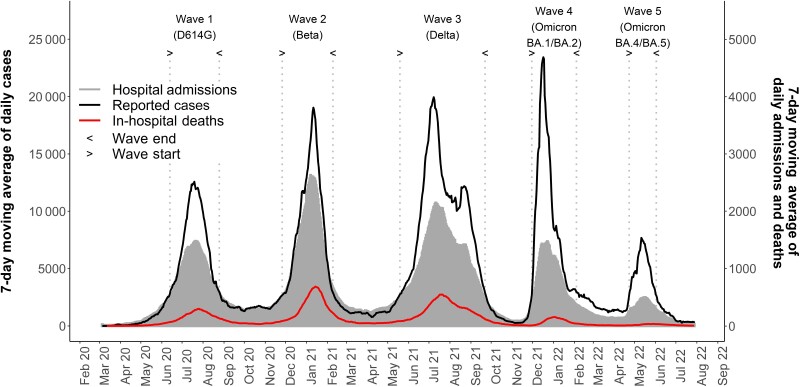
Background: In this study, we compared admission incidence risk and the risk of mortality in the Omicron BA.4/BA.5 wave to previous waves.
Methods: Data from South Africa's SARS-CoV-2 case linelist, national COVID-19 hospital surveillance system, and Electronic Vaccine Data System were linked and analyzed. Wave periods were defined when the country passed a weekly incidence of 30 cases/100 000 population. In-hospital case fatality ratios (CFRs) during the Delta, Omicron BA.1/BA.2, and Omicron BA.4/BA.5 waves were compared using post-imputation random effect multivariable logistic regression models.
Results: The CFR was 25.9% (N = 37 538 of 144 778), 10.9% (N = 6123 of 56 384), and 8.2% (N = 1212 of 14 879) in the Delta, Omicron BA.1/BA.2, and Omicron BA.4/BA.5 waves, respectively. After adjusting for age, sex, race, comorbidities, health sector, and province, compared with the Omicron BA.4/BA.5 wave, patients had higher risk of mortality in the Omicron BA.1/BA.2 wave (adjusted odds ratio [aOR], 1.3; 95% confidence interval [CI]: 1.2-1.4) and Delta wave (aOR, 3.0; 95% CI: 2.8-3.2). Being partially vaccinated (aOR, 0.9; 95% CI: .9-.9), fully vaccinated (aOR, 0.6; 95% CI: .6-.7), and boosted (aOR, 0.4; 95% CI: .4-.5) and having prior laboratory-confirmed infection (aOR, 0.4; 95% CI: .3-.4) were associated with reduced risks of mortality.
Conclusions: Overall, admission incidence risk and in-hospital mortality, which had increased progressively in South Africa's first 3 waves, decreased in the fourth Omicron BA.1/BA.2 wave and declined even further in the fifth Omicron BA.4/BA.5 wave. Mortality risk was lower in those with natural infection and vaccination, declining further as the number of vaccine doses increased.
Keywords: COVID-19; Omicron BA.4; Omicron BA.5; hospital admissions; mortality.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. S. S. A. K. reports grants or contracts unrelated to this work and paid to institution from the National Institutes of Health, South African Medical Research Council Cooperative Agreement, National Research Foundation/DST, USAID/Right to Care Cooperative agreement, the IQRAA Trust, and EDCTP; an unpaid role as a member of the World Health Organization (WHO) Science Council; a paid role as a member of the Bill and Melinda Gates Foundation (BMGF) Scientific Advisory Committee (meeting honorarium paid to author); and an unpaid role as vice-president of the International Science Council. C. C. reports grants or contracts unrelated to this work and paid to institution from the US Centers for Disease Control and Prevention (CDC), Wellcome Trust, Sanofi Pasteur, PATH, BMGF, and SA-Medical Research Council. A. v. G. reports grants unrelated to this work and paid to institution from the BMGF, Sanofi, CDC, WHO AFRO, Fleming Fund SEQAFRICA, SA MRC, the Solidarity Fund for Innovative Projects, NIH training grant, and ASLM PGI and a role as chair for the National Advisory Group for Immunisation. I. S. reports an institutional grant unrelated to this work from NIH DAIDS–WITS Helen Joseph Hospital CRS. M. J. G. reports grants or contracts unrelated to this work and paid to institution from the South African Medical Research Council and BMGF. N. W. reports grants paid to institution and unrelated to this work from the BMGF, Sanofi, and CDC. R. W. reports shareholding with Adcock Ingram Holdings Ltd, Dischem Pharmacies Ltd, Discovery Ltd, Netcare Ltd, and Aspen Pharmacare Holdings Ltd. S. W. reports grants unrelated to this work and paid to institution from the BMGF, Sanofi, CDC, and Welcome Trust. W. J. reports grants or contracts related to a long coronavirus disease 2019 study, paid to institution, from the BMGF. All remaining authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
