

Dropout from psychological treatment for borderline personality disorder: a multilevel survival meta-analysis
- PMID: 36453183
- PMCID: PMC9975988
- DOI: 10.1017/S0033291722003634
Dropout from psychological treatment for borderline personality disorder: a multilevel survival meta-analysis
Abstract
Background: Dropout from psychotherapy for borderline personality disorder (BPD) is a notorious problem. We investigated whether treatment, treatment format, treatment setting, substance use exclusion criteria, proportion males, mean age, country, and other variables influenced dropout.
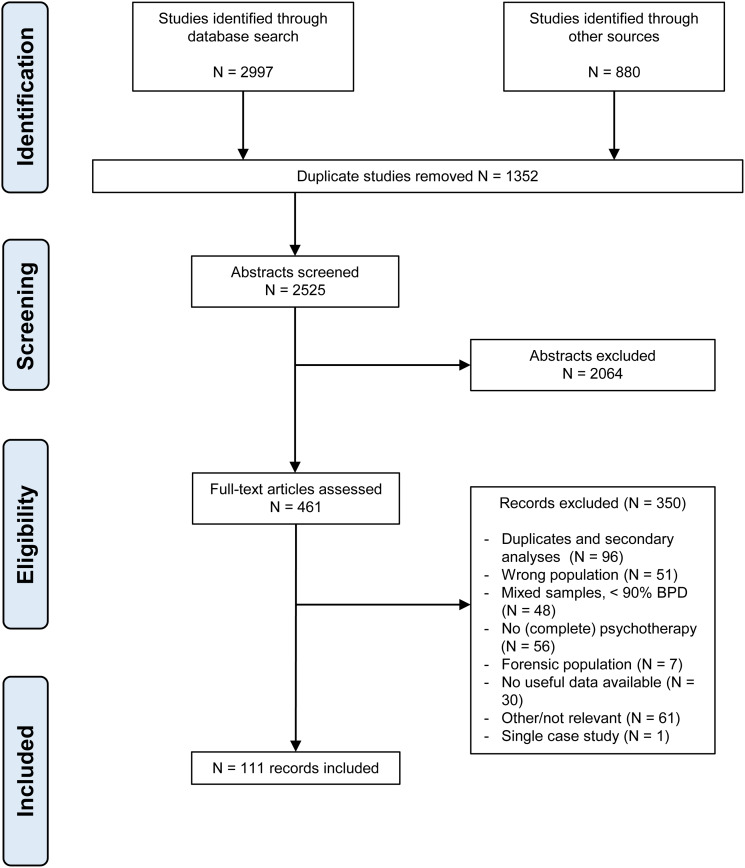
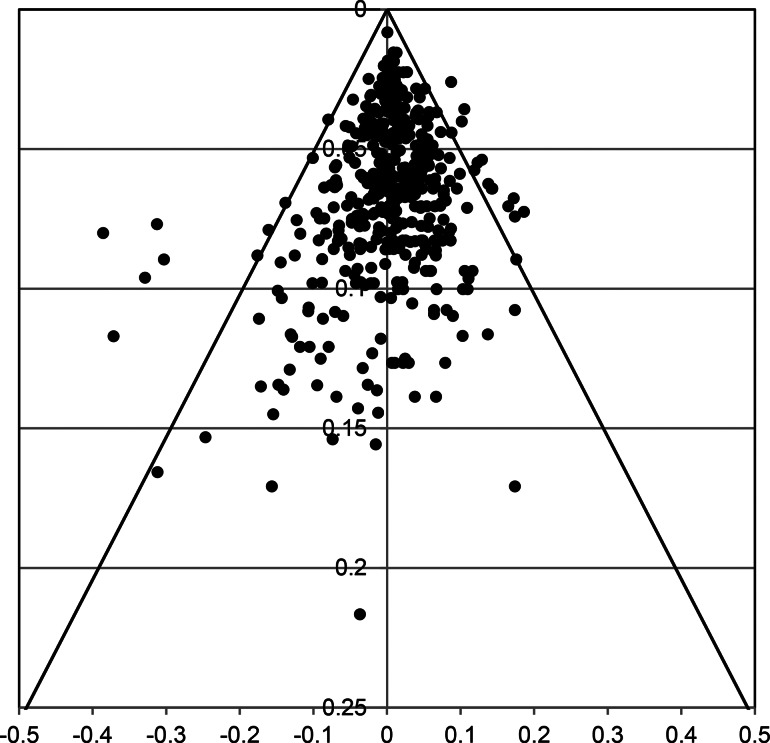
Methods: From Pubmed, Embase, Cochrane, Psycinfo and other sources, 111 studies (159 treatment arms, N = 9100) of psychotherapy for non-forensic adult patients with BPD were included. Dropout per quarter during one year of treatment was analyzed on participant level with multilevel survival analysis, to deal with multiple predictors, nonconstant dropout chance over time, and censored data. Multiple imputation was used to estimate quarter of drop-out if unreported. Sensitivity analyses were done by excluding DBT-arms with deviating push-out rules.
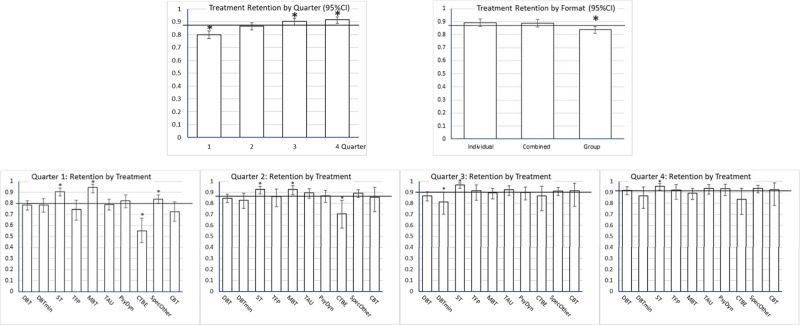
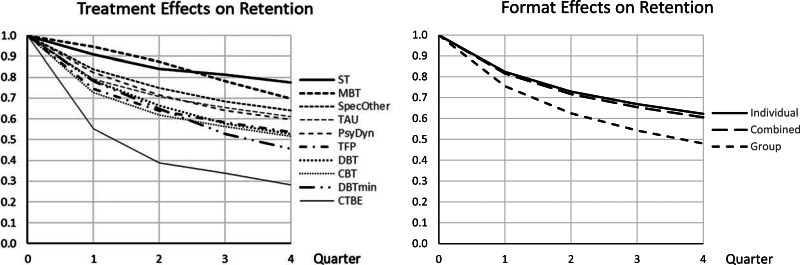
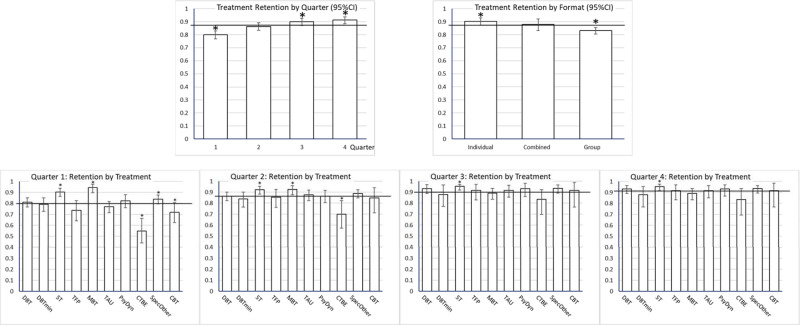
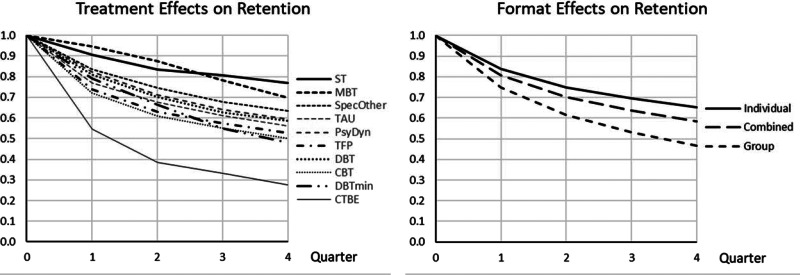
Results: Dropout was highest in the first quarter of treatment. Schema therapy had the lowest dropout overall, and mentalization-based treatment in the first two quarters. Community treatment by experts had the highest dropout. Moreover, individual therapy had lowest dropout, group therapy highest, with combined formats in-between. Other variables such as age or substance-use exclusion criteria were not associated with dropout.
Conclusion: The findings do not support claims that all treatments are equal, and indicate that efforts to reduce dropout should focus on early stages of treatment and on group treatment.
Keywords: Borderline personality disorder; dropout; meta-analysis; psychotherapy; treatment retention.
Figures
References
-
- Agresti, A., & Coull, B. A. (1998). Approximate is better than “exact” for interval estimation of binomial proportions. The American Statistician, 52(2), 119–126.
-
- American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
-
- Arntz, A., Jacob, G. A., Lee, C. W., Brand-de Wilde, O. M., Fassbinder, E., Harper, R. P., … Farrell, J. M. (2022). Effectiveness of predominantly group schema therapy and combined individual and group schema therapy for borderline personality disorder: A randomized clinical trial. JAMA Psychiatry, 79(4), 287–299. doi:10.1001/jamapsychiatry.2022.0010 - DOI - PMC - PubMed
-
- Arntz, A., Stupar-Rutenfrans, S., Bloo, J., van Dyck, R., & Spinhoven, P. (2015). Prediction of treatment discontinuation and recovery from borderline personality disorder: Results from an RCT comparing schema therapy and transference focused psychotherapy. Behaviour Research and Therapy, 74, 60–71. doi:10.1016/j.brat.2015.09.002 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
