Emergency application of extracorporeal membrane oxygenation in a pediatric case of sudden airway collapse due to anterior mediastinal mass: A case report and review of literature
- PMID: 36453783
- PMCID: PMC10198319
- DOI: 10.14744/tjtes.2021.49383
Emergency application of extracorporeal membrane oxygenation in a pediatric case of sudden airway collapse due to anterior mediastinal mass: A case report and review of literature
Abstract
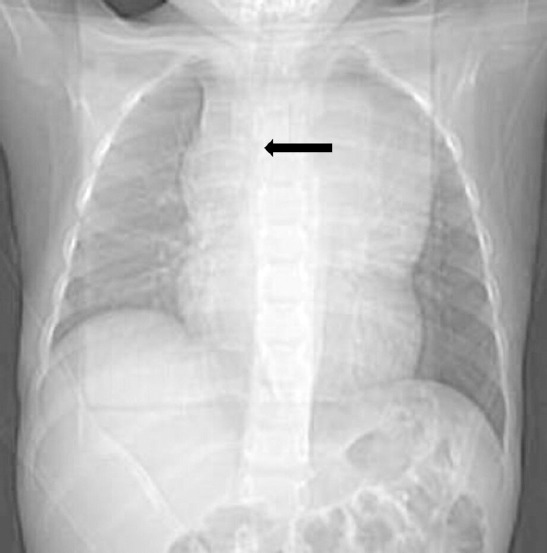
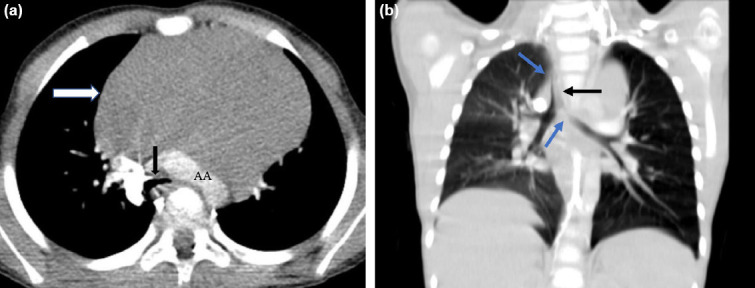
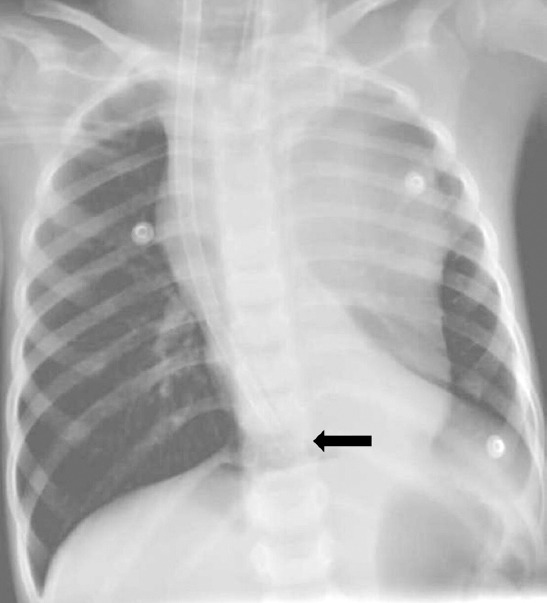
Mediastinal masses can compress the respiratory or cardiovascular system, especially when anteriorly located. Obtaining histological material for diagnosis poses a challenge due to the major risk of cardiorespiratory collapse following anesthetic procedure. Our case shows the utility of rescue with venovenous extracorporeal membrane oxygenation (VV-ECMO) after occurrence of such an event and demonstrates the feasibility of administering chemotherapy during VV-ECMO. A 4-year-old boy was referred to the pediatric oncology clinic of our hospital after a large mediastinal mass was observed on chest radiography ordered due to persistent cough. Computed tomography of the thorax revealed a 100×85 mm mass in the anterior mediastinum, surrounding the heart, and showed that there was compression to the trachea, bronchiole, and vascular structures. Percutaneous needle biopsy accompanied by ultrasonography was planned for diagnostic purposes. Low-dose ketamine and midazolam were administered for procedural sedation in the operating room. After the biopsy procedure, the patient developed sudden airway obstruction requiring intubation. Despite 100% oxygen support with a mechanical ventilator, pulse oximeter saturation remained below 80%. Chest X-ray revealed total collapse of the left lung, and the patient's oxygen saturation did not increase with selective left bronchial intubation. Bi-caval dual-lumen ECMO cannula was placed in the internal jugular vein and VV-ECMO was initiated, resulting in swift improvement in hypoxemia. The patients's anterior mediastinal mass shrank rapidly and left lung improved with chemotherapy. The patient remained on ECMO for a total of 9 days and was extubated 2 days after ECMO termination, followed by discharge to the pediatric oncology ward on the 20th day of pediatric intensive care unit stay. It is well known that large, anteriorly-located mediastinal masses carry a considerable risk of causing cardio-pulmonary collapse during procedures involving anesthesia. All life-saving options, including emergency ECMO, should be available before any planned invasive procedures in these patients.
Conflict of interest statement
Figures


References
-
- Linschoten M, Kamphuis JA, Van Rhenen A, Bosman LP, Cramer MJ, Doevendans PA, et al. Cardiovascular adverse events in patients with non-hodgkin lymphoma treated with first-line cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) or CHOP with rituximab (R-CHOP):A systematic review and meta-analysis. Lancet Haematol. 2020;7:e295–308. - PubMed
-
- Azarow KS, Pearl RH, Zurcher R, Edwards FH, Cohen AJ. Primary mediastinal masses:A comparison of adult and pediatric populations. J Thorac Cardiovasc Surg. 1993;106:67–72. - PubMed
-
- Lam JCM, Chui CH, Jacobsen AS, Tan AM, Joseph VT. When is a mediastinal mass critical in a child?An analysis of 29 patients. Pediatr Surg Int. 2004;20:180–4. - PubMed
-
- Blank RS, De Souza DG. Anesthetic management of patients with an anterior mediastinal mass:Continuing professional development. Can J Anaesth. 2011;58:853–9. - PubMed
-
- Luckhaupt-Koch K. Mediastinal mass syndrome. Paediatr Anaesth. 2005;15:437–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical