

Population-based correlates of COVID-19 infection: An analysis from the DFW COVID-19 prevalence study
- PMID: 36454745
- PMCID: PMC9714738
- DOI: 10.1371/journal.pone.0278335
Population-based correlates of COVID-19 infection: An analysis from the DFW COVID-19 prevalence study
Abstract
Background: COVID-19 has resulted in over 1 million deaths in the U.S. as of June 2022, with continued surges after vaccine availability. Information on related attitudes and behaviors are needed to inform public health strategies. We aimed to estimate the prevalence of COVID-19, risk factors of infection, and related attitudes and behaviors in a racially, ethnically, and socioeconomically diverse urban population.
Methods: The DFW COVID-19 Prevalence Study Protocol 1 was conducted from July 2020 to March 2021 on a randomly selected sample of adults aged 18-89 years, living in Dallas or Tarrant Counties, Texas. Participants were asked to complete a 15-minute questionnaire and COVID-19 PCR and antibody testing. COVID-19 prevalence estimates were calculated with survey-weighted data.
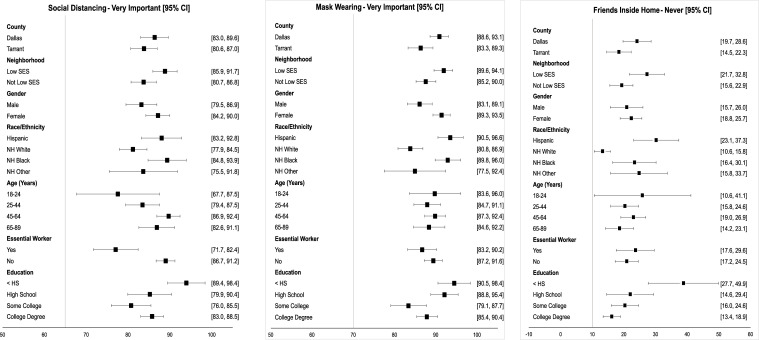
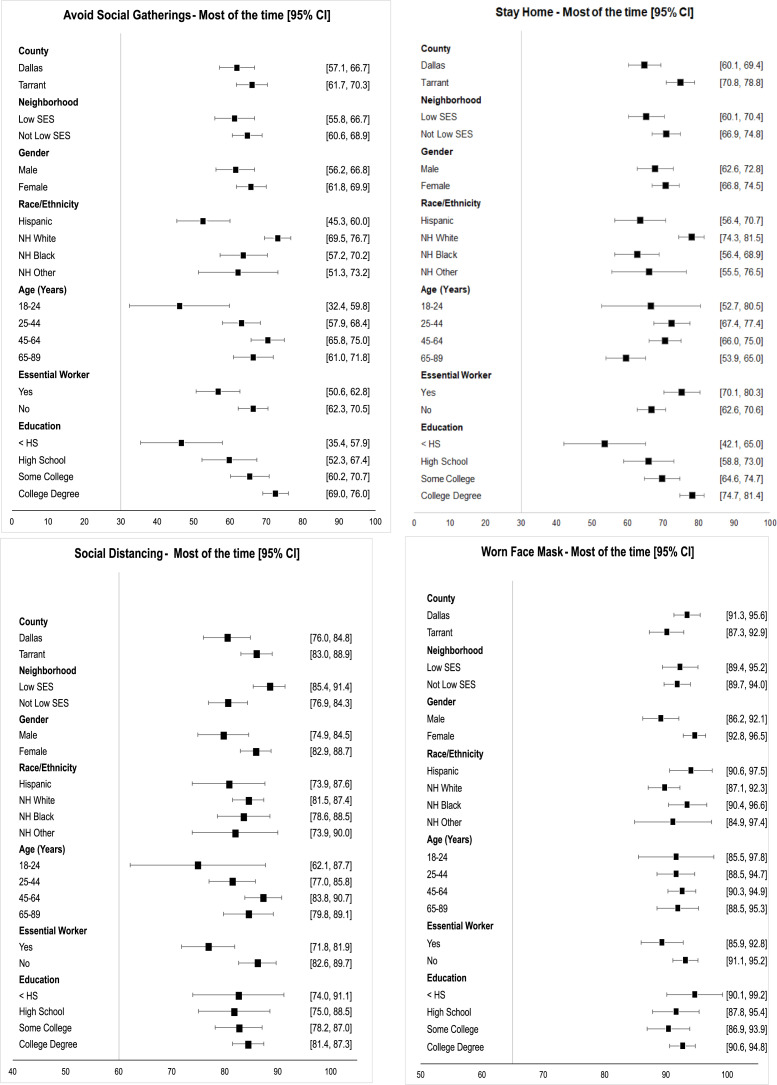
Results: Of 2969 adults who completed the questionnaire (7.4% weighted response), 1772 (53.9% weighted) completed COVID-19 testing. Overall, 11.5% of adults had evidence of COVID-19 infection, with a higher prevalence among Hispanic and non-Hispanic Black persons, essential workers, those in low-income neighborhoods, and those with lower education attainment compared to their counterparts. We observed differences in attitudes and behaviors by race and ethnicity, with non-Hispanic White persons being less likely to believe in the importance of mask wearing, and racial and ethnic minorities more likely to attend social gatherings.
Conclusion: Over 10% of an urban population was infected with COVID-19 early during the pandemic. Differences in attitudes and behaviors likely contribute to sociodemographic disparities in COVID-19 prevalence.
Copyright: © 2022 Singal et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Mohan BS, Nambiar V. COVID-19: An insight into SARS-CoV-2 pandemic originated at Wuhan City in Hubei Province of China. J Infect Dis Epidemiol. 2020;6: 146. doi: 10.23937/2474-3658/1510146 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
