

Face masks to prevent transmission of respiratory infections: Systematic review and meta-analysis of randomized controlled trials on face mask use
- PMID: 36454947
- PMCID: PMC9714953
- DOI: 10.1371/journal.pone.0271517
Face masks to prevent transmission of respiratory infections: Systematic review and meta-analysis of randomized controlled trials on face mask use
Erratum in
-
Correction: Face masks to prevent transmission of respiratory infections: Systematic review and meta-analysis of randomized controlled trials on face mask use.PLoS One. 2025 Mar 4;20(3):e0320226. doi: 10.1371/journal.pone.0320226. eCollection 2025. PLoS One. 2025. PMID: 40036174 Free PMC article.
-
Correction: Face masks to prevent transmission of respiratory infections: Systematic review and meta-analysis of randomized controlled trials on face mask use.PLoS One. 2025 May 30;20(5):e0325466. doi: 10.1371/journal.pone.0325466. eCollection 2025. PLoS One. 2025. PMID: 40445874 Free PMC article.
Abstract
Objectives: To examine the use of face mask intervention in mitigating the risk of spreading respiratory infections and whether the effect of face mask intervention differs in different exposure settings and age groups.
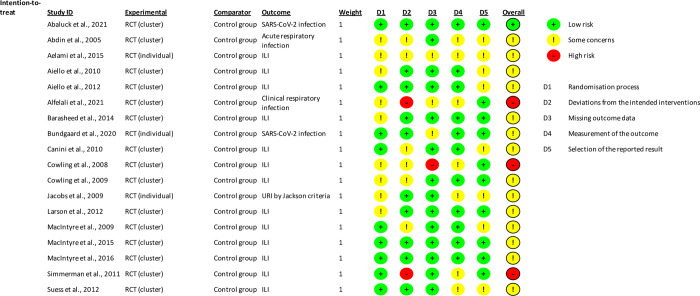
Design: Systematic review and meta-analysis. We evaluated the risk of bias using the Cochrane Risk of Bias 2 tool (ROB2).
Data sources: We searched PubMed, Embase, Cochrane Central Register of Controlled Trials, and Web of Science were searched for randomized controlled trials investigating the effect of face masks on respiratory infections published between 1981 and February 9, 2022. We followed the PRISMA 2020 guidelines.
Eligibility criteria for selecting studies: We included randomized controlled trials investigating the use of face mask intervention in mitigating the risk of spreading respiratory infections across different exposure settings.
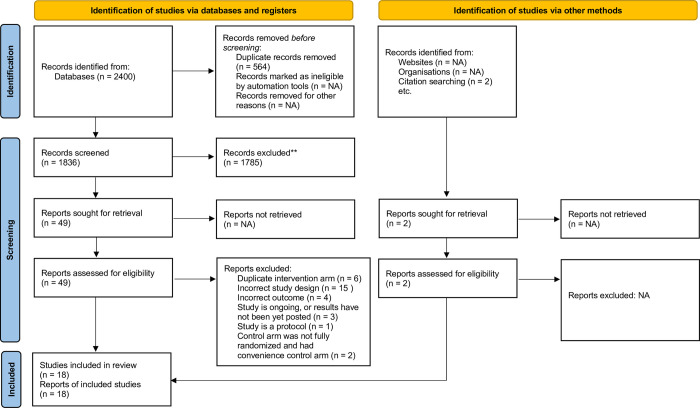
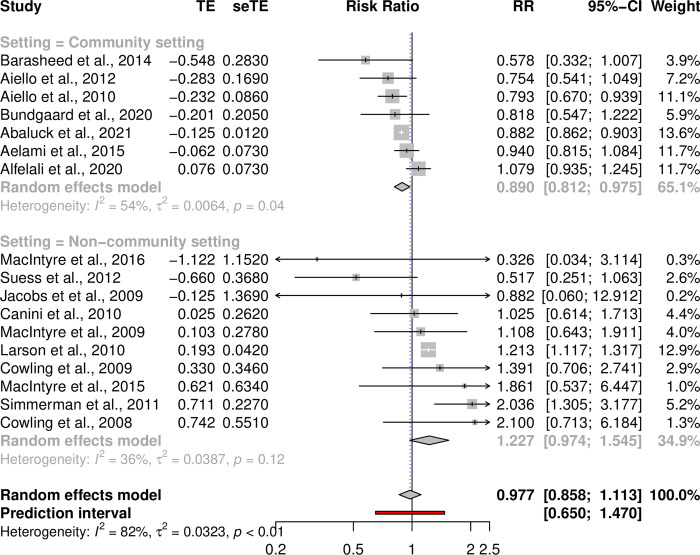
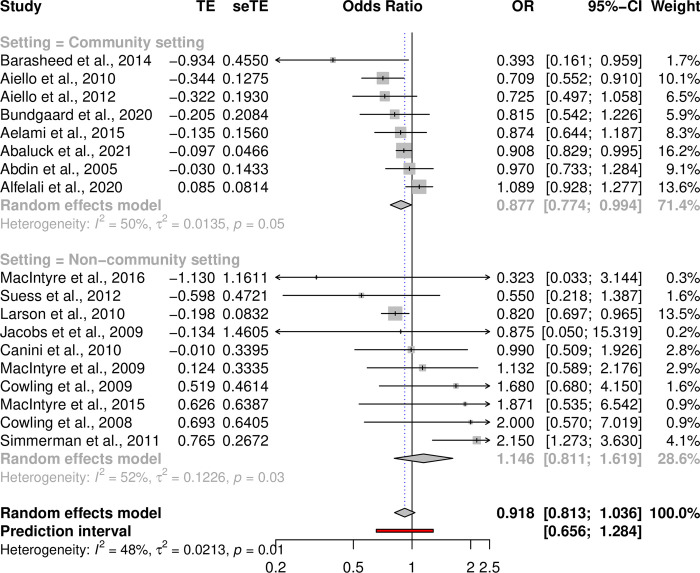
Results: We identified 2,400 articles for screening. 18 articles passed the inclusion criteria for both evidence synthesis and meta-analysis. There were N = 189,145 individuals in the face mask intervention arm and N = 173,536 in the control arm, and the follow-up times ranged from 4 days to 19 months. Our results showed between-study heterogeneity (p < 0.0001). While there was no statistically significant association over all studies when the covariate unadjusted intervention effect estimates were used (RR = 0.977 [0.858-1.113], p = 0.728), our subgroup analyses revealed that a face mask intervention reduced respiratory infections in the adult subgroup (RR = 0.8795 [0.7861-0.9839], p = 0.0249) and in a community setting (RR = 0.890 [0.812-0.975], p = 0.0125). Furthermore, our leave-one-out analysis found that one study biased the results towards a null effect. Consequently, when using covariate adjusted odds ratio estimates to have a more precise effect estimates of the intervention effect to account for differences at the baseline, the results showed that a face mask intervention did reduce respiratory infections when the biasing study was excluded from the analysis (OR = 0.8892 [0.8061-0.9810], p = 0.0192).
Conclusion: Our findings support the use of face masks particularly in a community setting and for adults. We also observed substantial between-study heterogeneity and varying adherence to protocol. Notably, many studies were subject to contamination bias thus affecting the efficacy of the intervention, that is when also some controls used masks or when the intervention group did not comply with mask use leading to a downward biased effect of treatment receipt and efficacy.
Trial registration: PROSPERO registration number CRD42020205523.
Copyright: © 2022 Ollila et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Murray E.J. , Epidemiology’s Time of Need: COVID-19 Calls for Epidemic-Related Economics. Journal of Economic Perspectives, 2020. 34(4): p. 105–20.
-
- Organization, W.H., Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). 2020.
-
- Sharma S.K., et al., COVID–19: Guidance Outlines on Infection Prevention and Control for Health Care Workers. Indian Journal of Community Health, 2020. 32(1): p. 8–14.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
