

The spectrum of GATA2 deficiency syndrome
- PMID: 36455197
- PMCID: PMC10082373
- DOI: 10.1182/blood.2022017764
The spectrum of GATA2 deficiency syndrome
Abstract
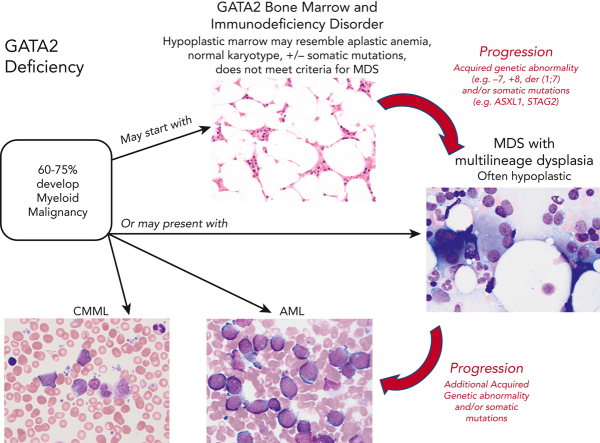
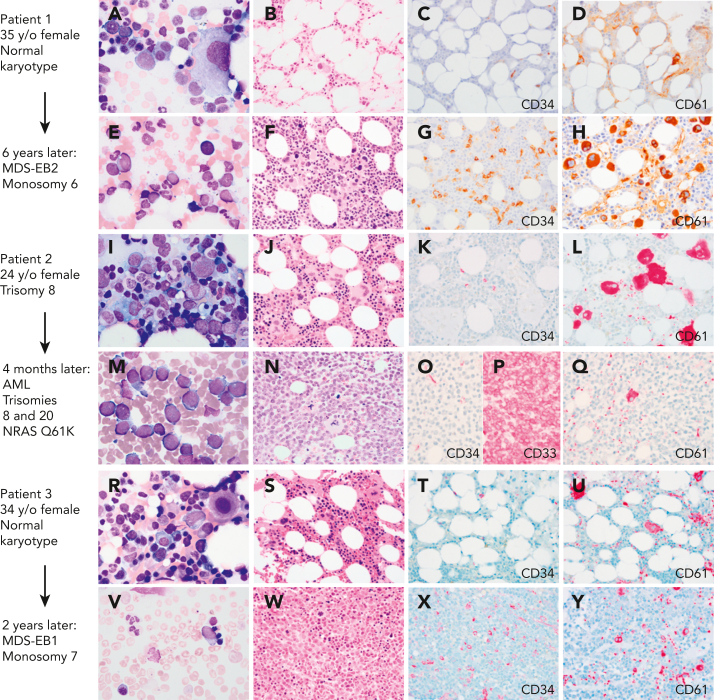
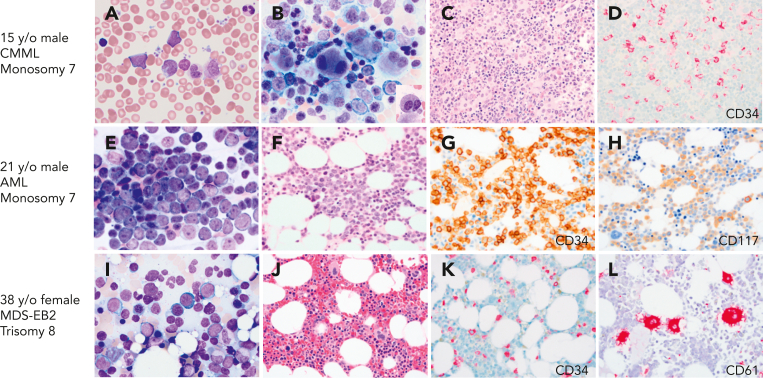
Inherited or de novo germ line heterozygous mutations in the gene encoding the transcription factor GATA2 lead to its deficiency. This results in a constellation of clinical features including nontuberculous mycobacterial, bacterial, fungal, and human papillomavirus infections, lymphedema, pulmonary alveolar proteinosis, and myelodysplasia. The onset, or even the presence, of disease is highly variable, even in kindreds with the identical mutation in GATA2. The clinical manifestations result from the loss of a multilineage progenitor that gives rise to B lymphocytes, monocytes, natural killer cells, and dendritic cells, leading to cytopenias of these lineages and subsequent infections. The bone marrow failure is typically characterized by hypocellularity. Dysplasia may either be absent or subtle but typically evolves into multilineage dysplasia with prominent dysmegakaryopoiesis, followed in some instances by progression to myeloid malignancies, specifically myelodysplastic syndrome, acute myelogenous leukemia, and chronic myelomonocytic leukemia. The latter 3 malignancies often occur in the setting of monosomy 7, trisomy 8, and acquired mutations in ASXL1 or in STAG2. Importantly, myeloid malignancy may represent the primary presentation of disease without recognition of other syndromic features. Allogeneic hematopoietic stem cell transplantation (HSCT) results in reversal of the phenotype. There remain important unanswered questions in GATA2 deficiency, including the following: (1) Why do some family members remain asymptomatic despite harboring deleterious mutations in GATA2? (2) What are the genetic changes that lead to myeloid progression? (3) What causes the apparent genetic anticipation? (4) What is the role of preemptive HSCT?
Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
Comment in
-
Introduction to a review series on germ line predisposition to hematologic malignancies: time to consider germ line testing.Blood. 2023 Mar 30;141(13):1509-1512. doi: 10.1182/blood.2023019846. Blood. 2023. PMID: 36787501 No abstract available.
References
-
- Mansour S, Connell F, Steward C, et al. Emberger syndrome—primary lymphedema with myelodysplasia: report of seven new cases. Am J Med Genet. 2010;152A(9):2287–2296. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
