

Palliated Hypoplastic Left Heart Syndrome Patients Experience Superior Waitlist and Comparable Post-Heart Transplant Survival to Non-Single Ventricle Congenital Heart Disease Patients
- PMID: 36455711
- PMCID: PMC10225473
- DOI: 10.1053/j.semtcvs.2022.08.019
Palliated Hypoplastic Left Heart Syndrome Patients Experience Superior Waitlist and Comparable Post-Heart Transplant Survival to Non-Single Ventricle Congenital Heart Disease Patients
Abstract
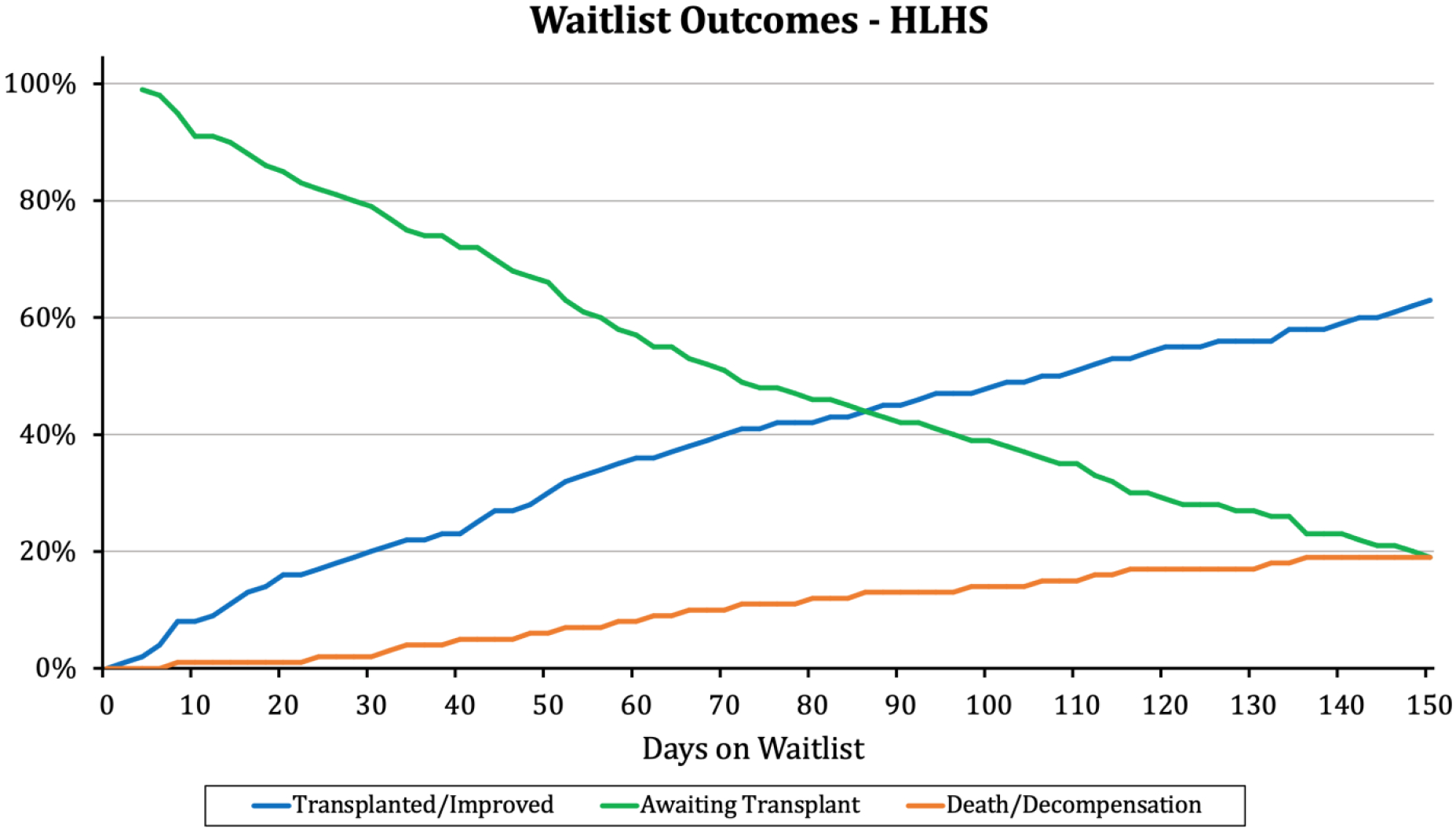
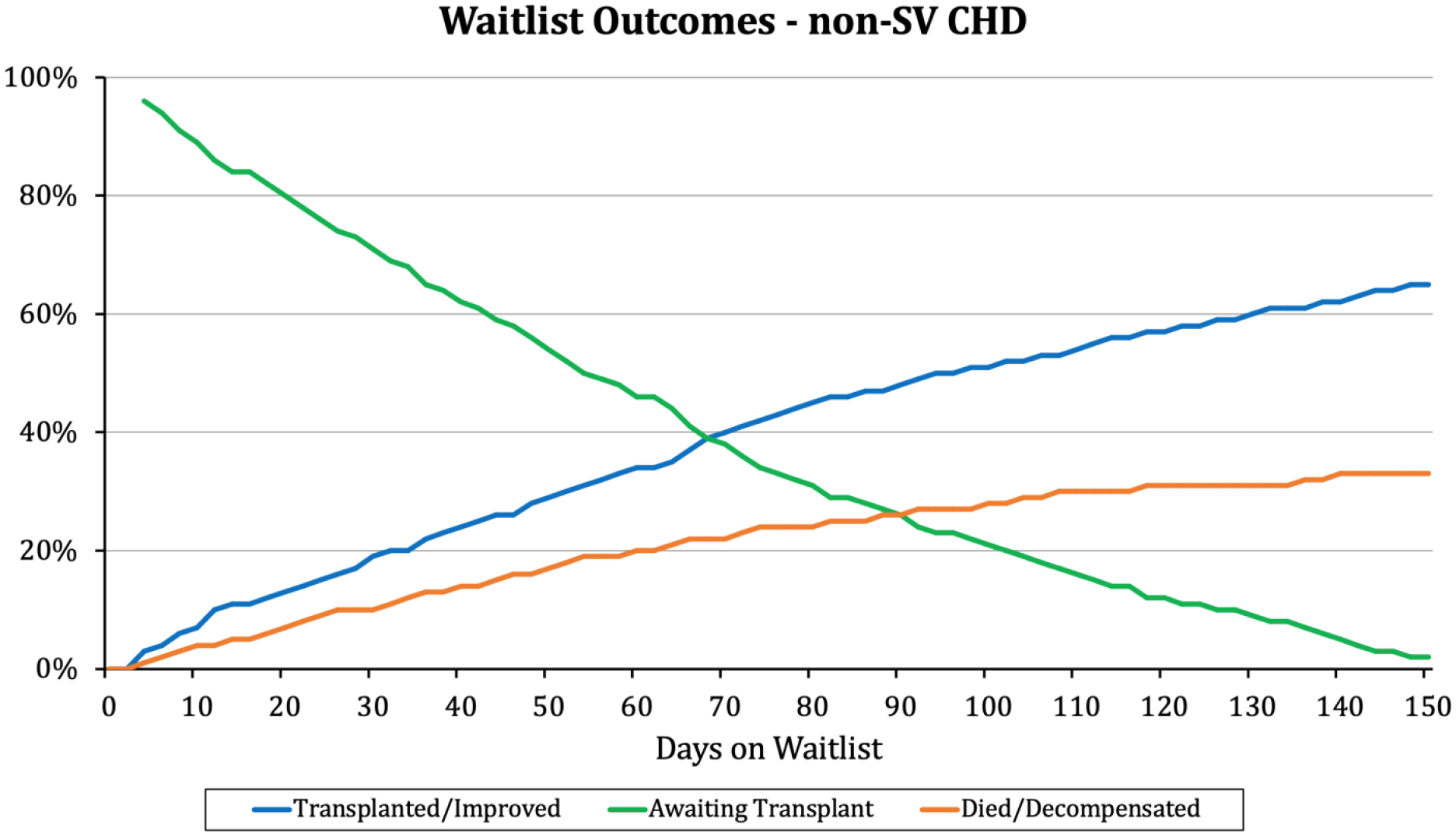
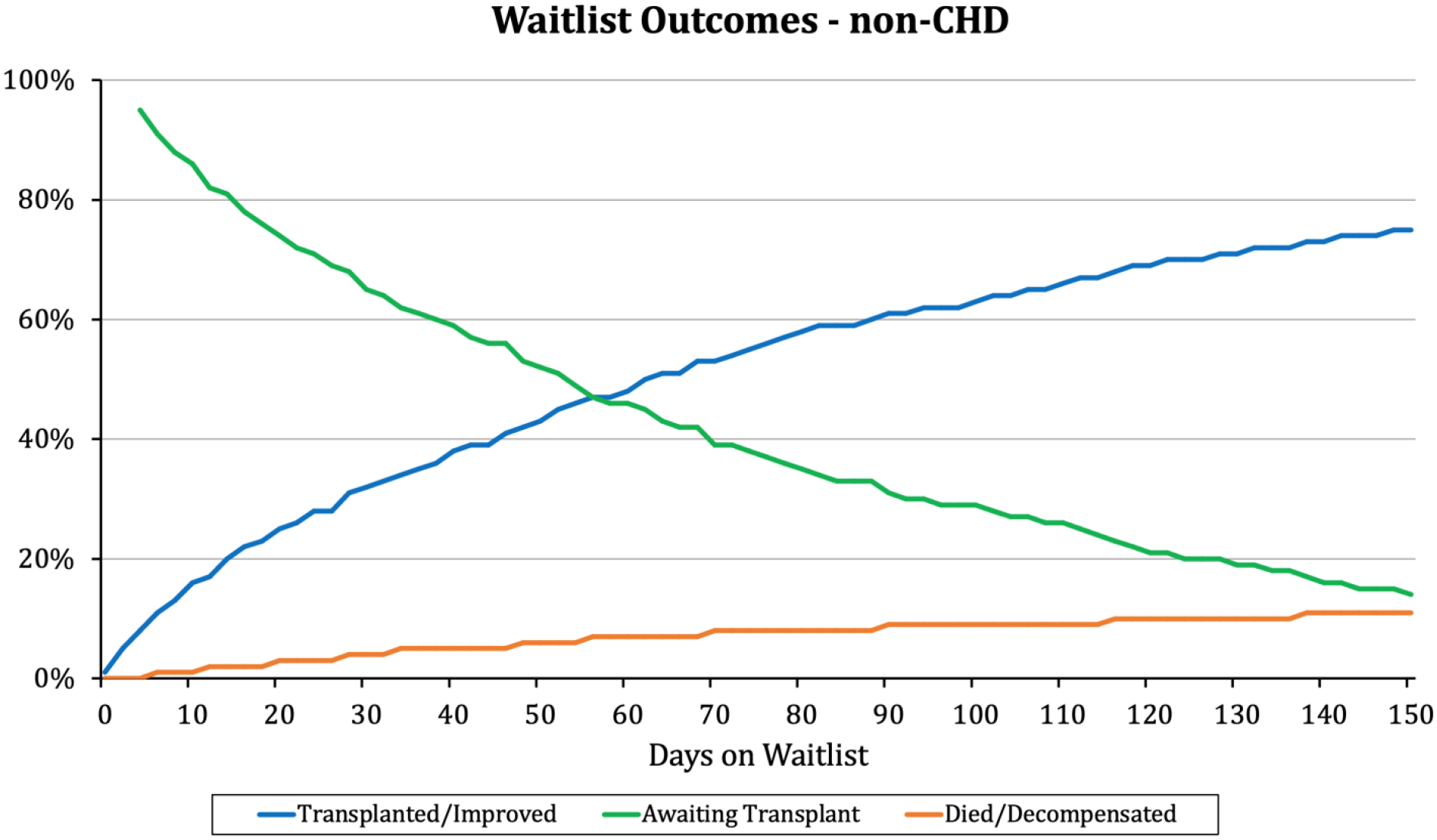
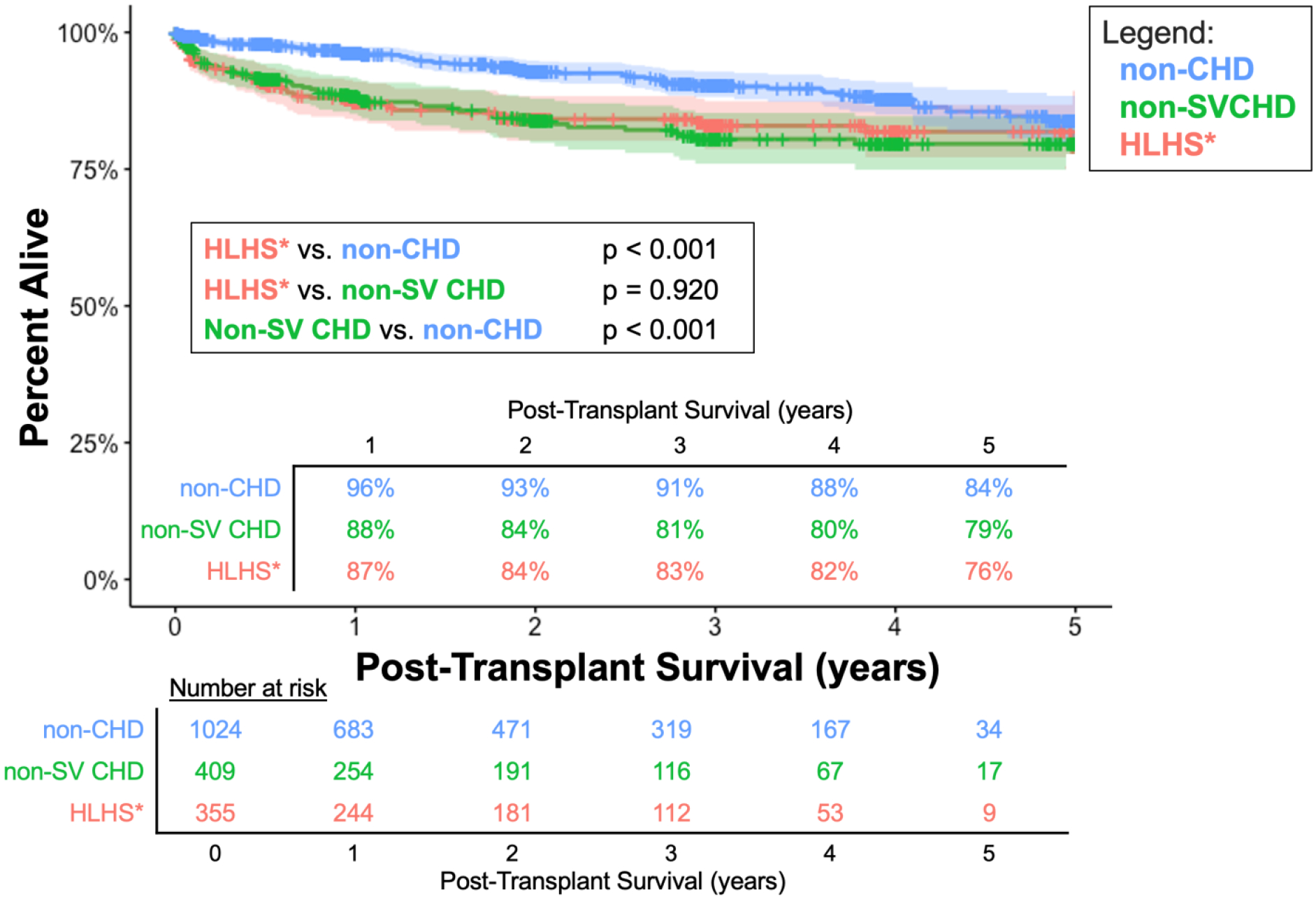
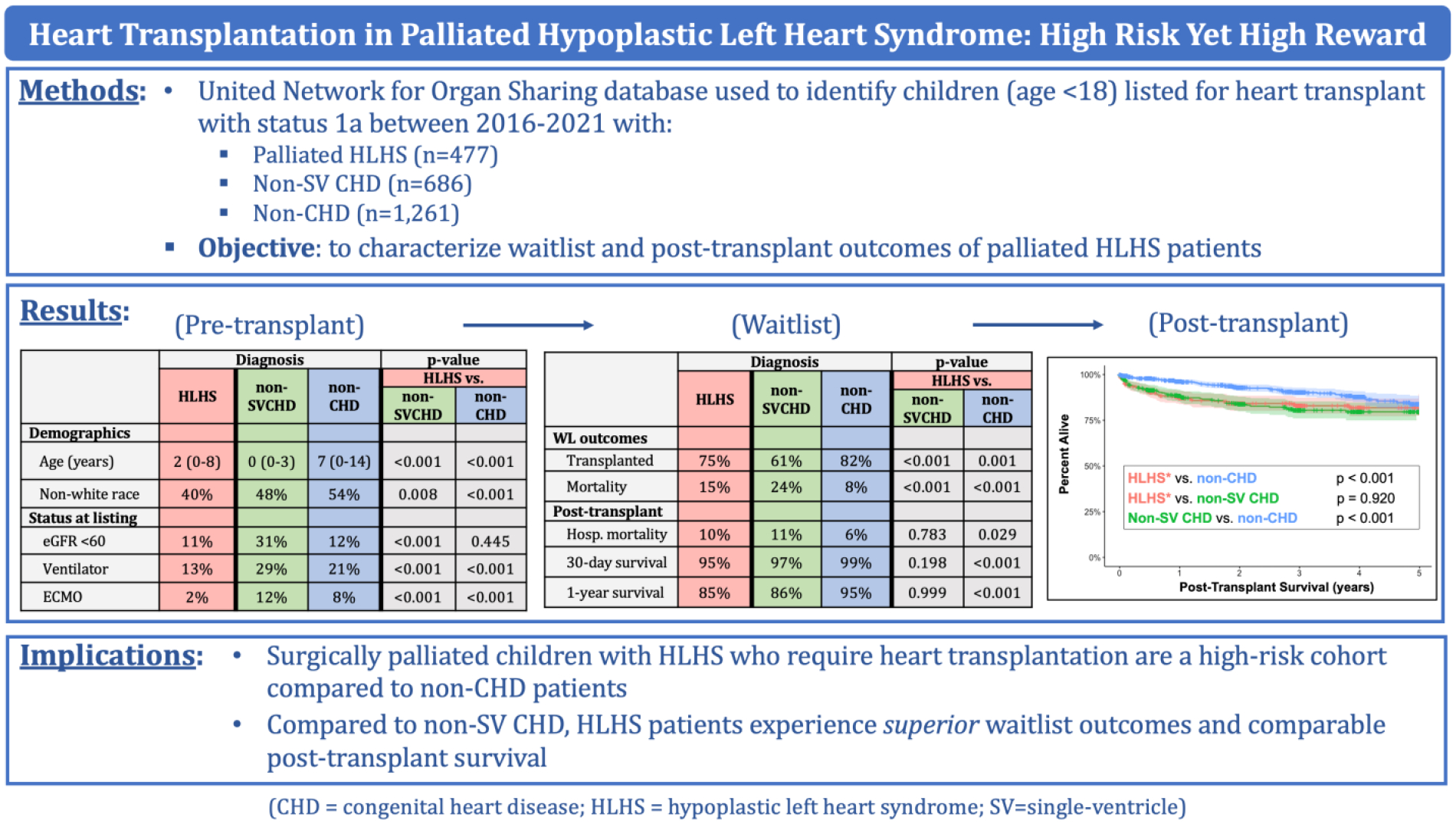
Congenital heart disease (CHD) is a well-established risk factor for inferior waitlist and post-heart transplant survival in children. Differences in outcomes between CHD subgroups are understudied. The present study compared outcomes for palliated hypoplastic left heart syndrome (HLHS) patients to other non-single ventricle CHD (non-SVCHD) and non-CHD patients. United Network for Organ Sharing was used to identify children (age < 18) listed for heart transplant in the United States between 2016 and 2021. CHD sub-diagnoses were only available for United Network for Organ Sharing status 1a after 2015, thereby defining the cohort. Waitlist outcomes were studied using competing-risk time-to-event analysis for transplantation, mortality/decompensation, and alive-on-waitlist. Multivariable Cox proportional hazards regression analyses were used to identify factors associated with inferior post-transplant survival. Patients included: palliated-HLHS (n = 477), non-SVCHD (n = 686), and non-CHD (n = 1261). At listing, Palliated-HLHS patients were older than non-SVCHD (median 2-year [IQR 0-8] vs median 0-year [0-3], respectively) and younger than non-CHD (median 7-year [0-14]) (P < 0.001 vs both), and were more likely to be white (P < 0.01 vs both). Upon time-to-event analysis, rates of waitlist mortality/decompensation rates were greater among non-SVCHD than palliated-HLHS. Post-transplant survival was comparable between palliated-HLHS and non-SVCHD (P = 0.920) but worse compared to non-CHD (P < 0.001). Both palliated-HLHS (HR 2.40 [95% CI 1.68-3.42]) and non-SVSCHD (2.04 [1.39-2.99]) were independently associated with post-transplant mortality. Palliated-HLHS patients with heart failure experience significantly worse post-transplant outcomes than non-CHD but, compared to other CHD patients, experience superior waitlist and comparable post-transplant survival. While a high-risk cohort, HLHS patients can achieve gratifying waitlist and post-transplant survival.
Keywords: Clinical outcomes; Congenital cardiac surgery; Congenital heart disease; Heart transplantation; Hypoplastic left heart syndrome; Norwood procedure; Quality improvement.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Long-Term Survival and Patient-Reported Outcomes After Staged Reconstructive Surgery for Hypoplastic Left Heart Syndrome.J Am Coll Cardiol. 2025 Jun 24;85(24):2386-2398. doi: 10.1016/j.jacc.2025.04.028. J Am Coll Cardiol. 2025. PMID: 40533128
-
Superior Waitlist Outcomes Among Patients Listed for Donation After Circulatory Death Heart Transplantation.JACC Heart Fail. 2025 Aug;13(8):102495. doi: 10.1016/j.jchf.2025.03.039. Epub 2025 Jun 16. JACC Heart Fail. 2025. PMID: 40527153
-
Machine Learning for Predicting Waitlist Mortality in Pediatric Heart Transplantation.Pediatr Transplant. 2025 Jun;29(4):e70095. doi: 10.1111/petr.70095. Pediatr Transplant. 2025. PMID: 40289835 Free PMC article.
-
Evaluation of the ventricular assist device programme in the UK.Health Technol Assess. 2006 Nov;10(48):1-119, iii-iv. doi: 10.3310/hta10480. Health Technol Assess. 2006. PMID: 17134596
-
Palivizumab for immunoprophylaxis of respiratory syncytial virus (RSV) bronchiolitis in high-risk infants and young children: a systematic review and additional economic modelling of subgroup analyses.Health Technol Assess. 2011 Jan;15(5):iii-iv, 1-124. doi: 10.3310/hta15050. Health Technol Assess. 2011. PMID: 21281564 Free PMC article.
Cited by
-
Human Stem Cell-Derived Cardiomyocytes Integrate Into the Heart of Monkeys With Right Ventricular Pressure Overload.Cell Transplant. 2024 Jan-Dec;33:9636897241290367. doi: 10.1177/09636897241290367. Cell Transplant. 2024. PMID: 39487759 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
