

Prognostic factors for streptococcal toxic shock syndrome: systematic review and meta-analysis
- PMID: 36456018
- PMCID: PMC9716873
- DOI: 10.1136/bmjopen-2022-063023
Prognostic factors for streptococcal toxic shock syndrome: systematic review and meta-analysis
Abstract
Objectives: To quantify the prognostic effects of demographic and modifiable factors in streptococcal toxic shock syndrome (STSS).
Design: Systematic review and meta-analysis.
Data sources: MEDLINE, EMBASE and CINAHL from inception to 19 September 2022, along with citations of included studies.
Eligibility criteria: Pairs of reviewers independently screened potentially eligible studies of patients with Group A Streptococcus-induced STSS that quantified the association between at least one prognostic factor and outcome of interest.
Data extraction and synthesis: We performed random-effects meta-analysis after duplicate data extraction and risk of bias assessments. We rated the certainty of evidence using the Grading of Recommendations, Assessment, Development and Evaluation approach.
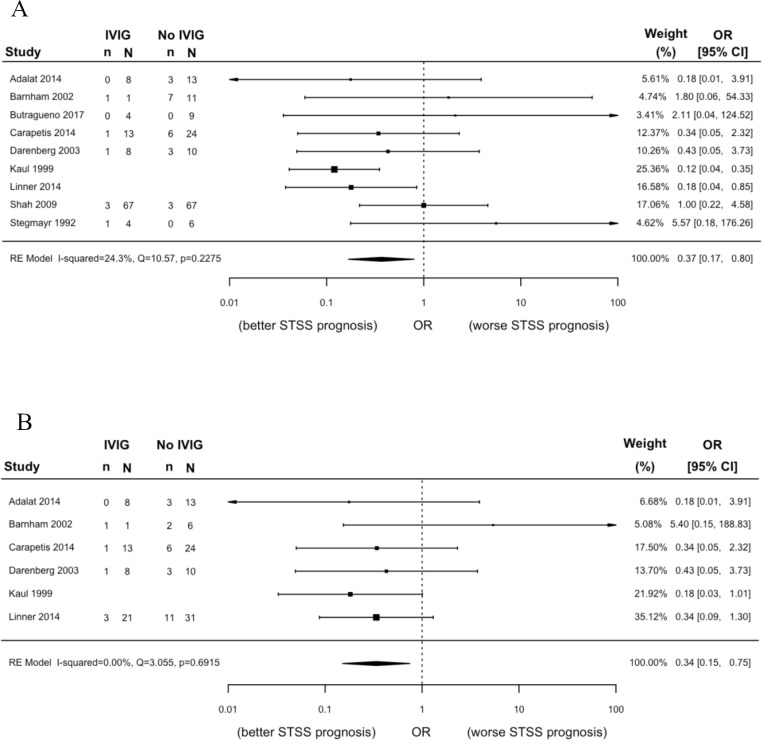
Results: One randomised trial and 40 observational studies were eligible (n=1918 patients). We found a statistically significant association between clindamycin treatment and mortality (n=144; OR 0.14, 95% CI 0.06 to 0.37), but the certainty of evidence was low. Within clindamycin-treated STSS patients, we found a statistically significant association between intravenous Ig treatment and mortality (n=188; OR 0.34, 95% CI 0.15 to 0.75), but the certainty of evidence was also low. The odds of mortality may increase in patients ≥65 years when compared with patients 18-64 years (n=396; OR 2.37, 95% CI 1.47 to 3.84), but the certainty of evidence was low. We are uncertain whether non-steroidal anti-inflammatory drugs increase the odds of mortality (n=50; OR 4.14, 95% CI 1.13 to 15.14; very low certainty). Results failed to show a significant association between any other prognostic factor and outcome combination (very low to low certainty evidence) and no studies quantified the association between a prognostic factor and morbidity post-infection in STSS survivors.
Conclusions: Treatment with clindamycin and within clindamycin-treated patients, IVIG, was each significantly associated with mortality, but the certainty of evidence was low. Future research should focus on morbidity post-infection in STSS survivors.
Prospero registration number: CRD42020166961.
Keywords: bacteriology; epidemiology; general medicine (see internal medicine).
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ML declares grants or contracts from the WHO, consulting fees from AVIR Pharma, and participating on data safety monitoring or advisory boards for Paladin Labs and Sunovion Pharmaceuticals.
Figures
References
-
- Canada Go. Group A streptococcal diseases: for health professionals, 2019. Available: https://www.canada.ca/en/public-health/services/diseases/group-a-strepto...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical