

Use of Rituximab in Childhood Idiopathic Nephrotic Syndrome
- PMID: 36456193
- PMCID: PMC10103321
- DOI: 10.2215/CJN.08570722
Use of Rituximab in Childhood Idiopathic Nephrotic Syndrome
Abstract
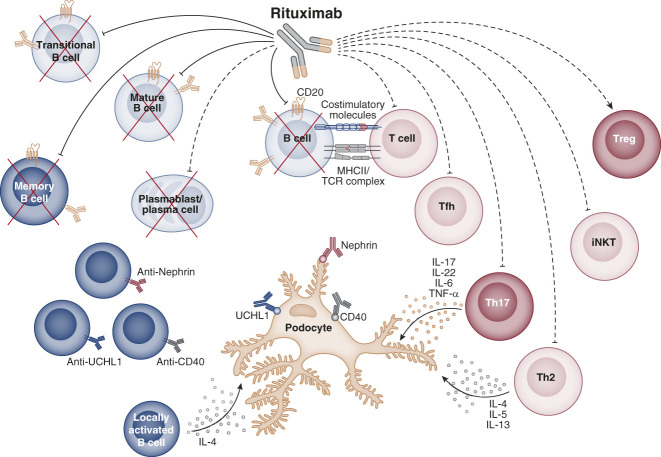
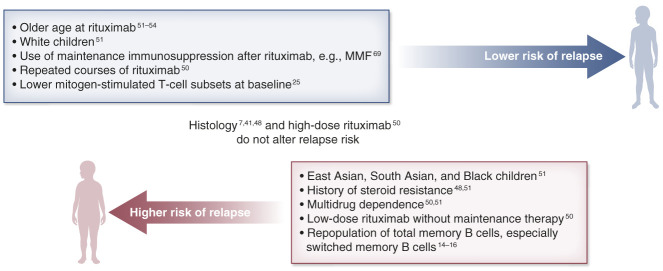
Rituximab is an established therapy in children with idiopathic nephrotic syndrome to sustain short- to medium-term disease remission and avoid steroid toxicities. Recent trials focus on its use as a first-line agent among those with milder disease severity. Rituximab is used in multidrug refractory nephrotic syndrome and post-transplant disease recurrence, although the evidence is much less substantial. Available data suggest that the treatment response to rituximab depends on various patient factors, dosing regimen, and the concomitant use of maintenance immunosuppression. After repeated treatments, patients are found to have an improving response overall with a longer relapse-free period. The drug effect, however, is not permanent, and 80% of patients eventually relapse and many will require an additional course of rituximab. This underpins the importance of understanding the long-term safety profile on repeated treatments. Although rituximab appears to be generally safe, there are concerns about long-term hypogammaglobulinemia, especially in young children. Reliable immunophenotyping and biomarkers are yet to be discovered to predict treatment success, risk of both rare and severe side effects, e.g. , persistent hypogammaglobulinemia, and guiding of redosing strategy. In this review, we highlight recent advances in the use of rituximab for childhood nephrotic syndrome and how the therapeutic landscape is evolving.
Trial registration: ClinicalTrials.gov NCT03560011 NCT03899103.
Copyright © 2022 by the American Society of Nephrology.
Conflict of interest statement
M. Colucci reports other interests or relationships with Italian Ministry of Health (5 x mille), Fondazione Bambino Gesú and Associazione per la Cura del Bambino Nefropatico ONLUS. R.S. Parekh reports ownership interest in Coramed-stock, SpineFx, and Synaptive-stock; research funding from Canadian Institute of Health Research (CIHR), NIH, and Ontario Ministry; patents or royalties from IZI and SpineFx; serving as an Associate Editor of
Figures
References
-
- Iijima K, Sako M, Nozu K, et al. Rituximab for childhood-onset, complicated, frequently relapsing nephrotic syndrome or steroid-dependent nephrotic syndrome: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet. 2014;384(9950):1273–1281. doi:10.1016/s0140-6736(14)60541-9 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
