

Improving head and neck cancer therapies by immunomodulation of the tumour microenvironment
- PMID: 36456755
- PMCID: PMC9992112
- DOI: 10.1038/s41568-022-00531-9
Improving head and neck cancer therapies by immunomodulation of the tumour microenvironment
Abstract
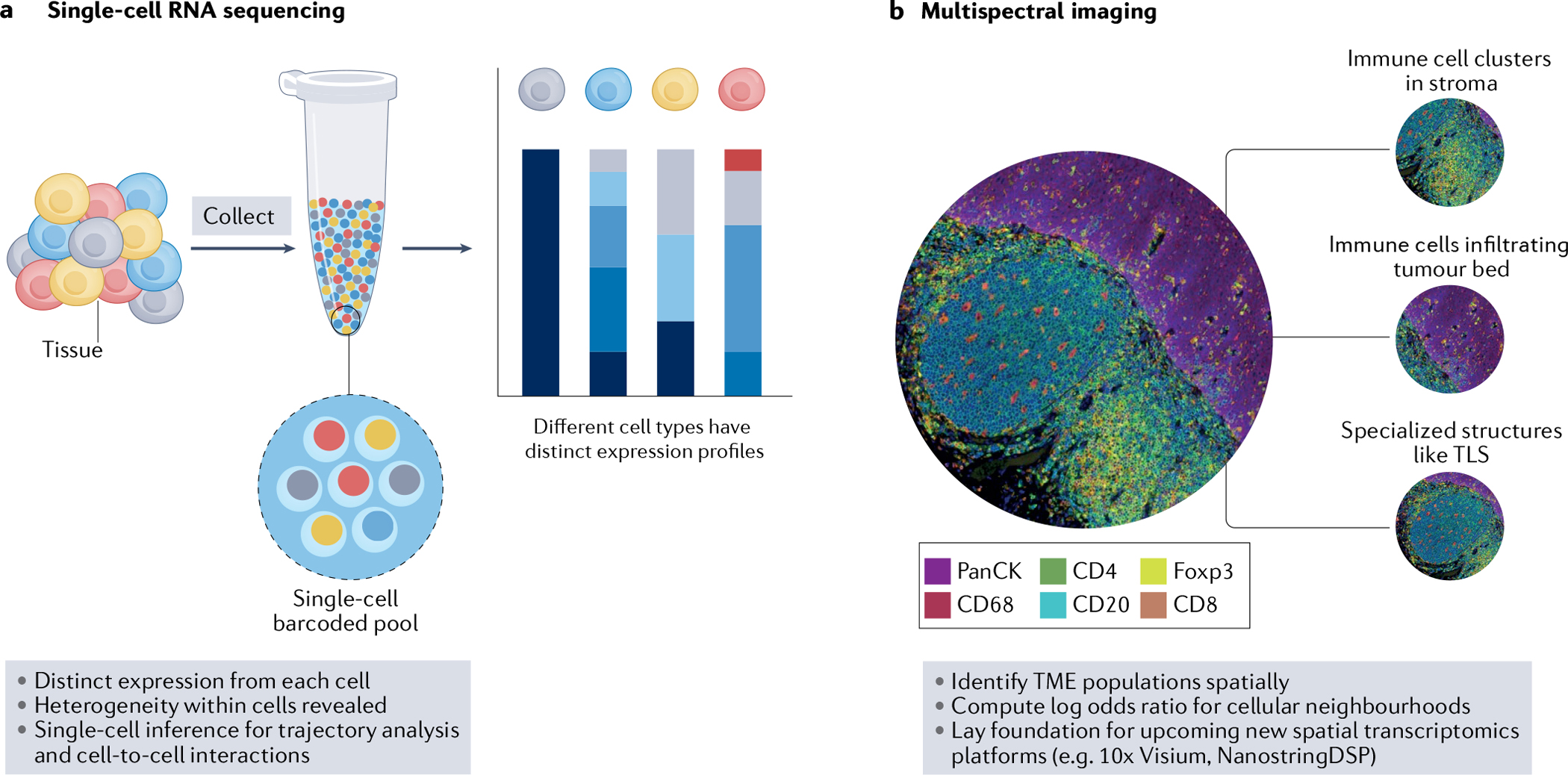
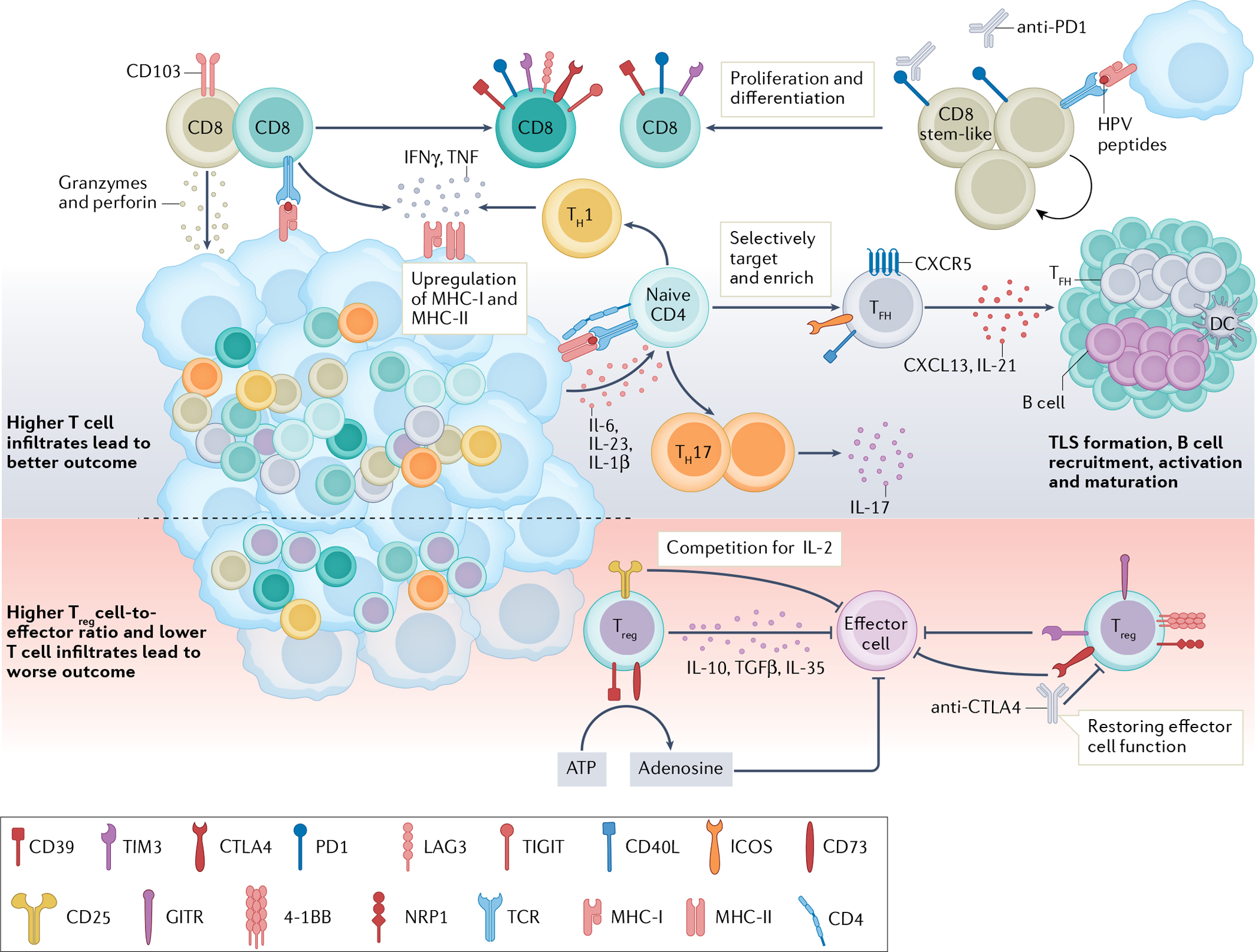
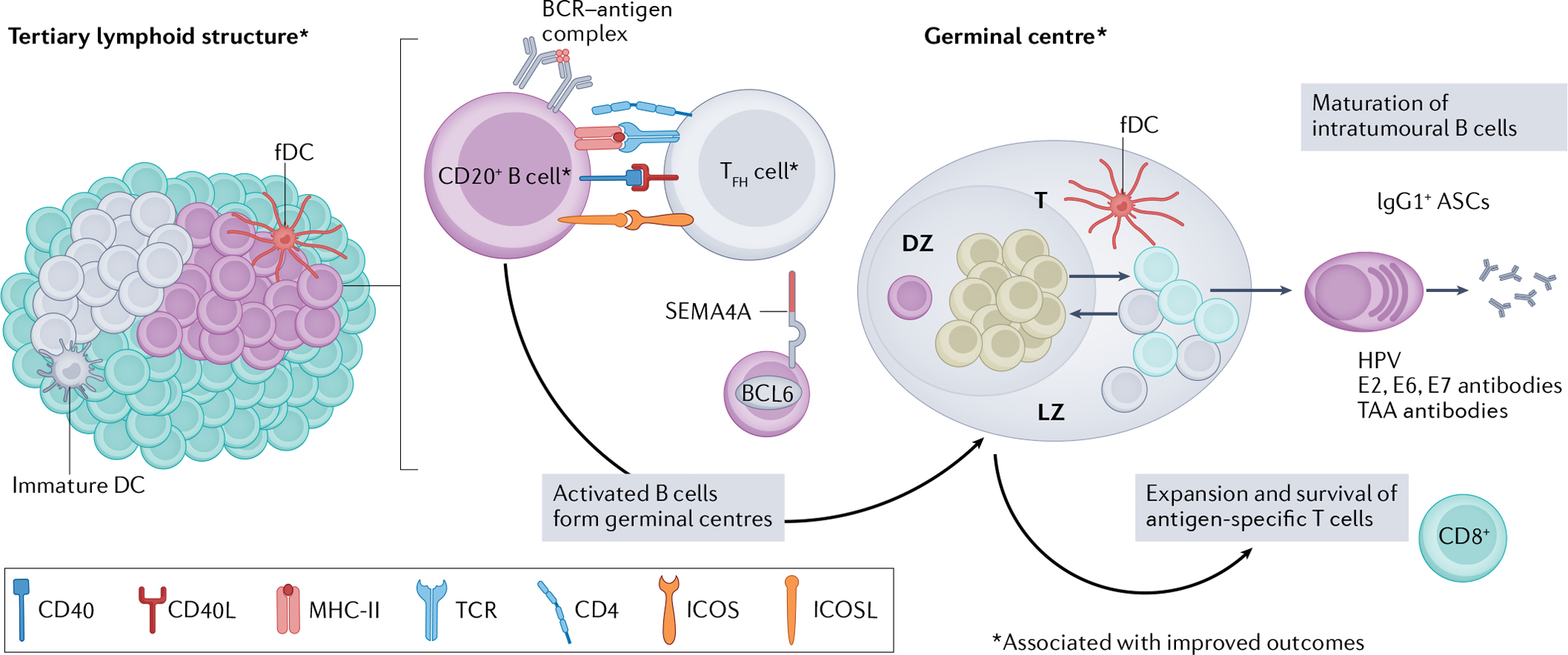
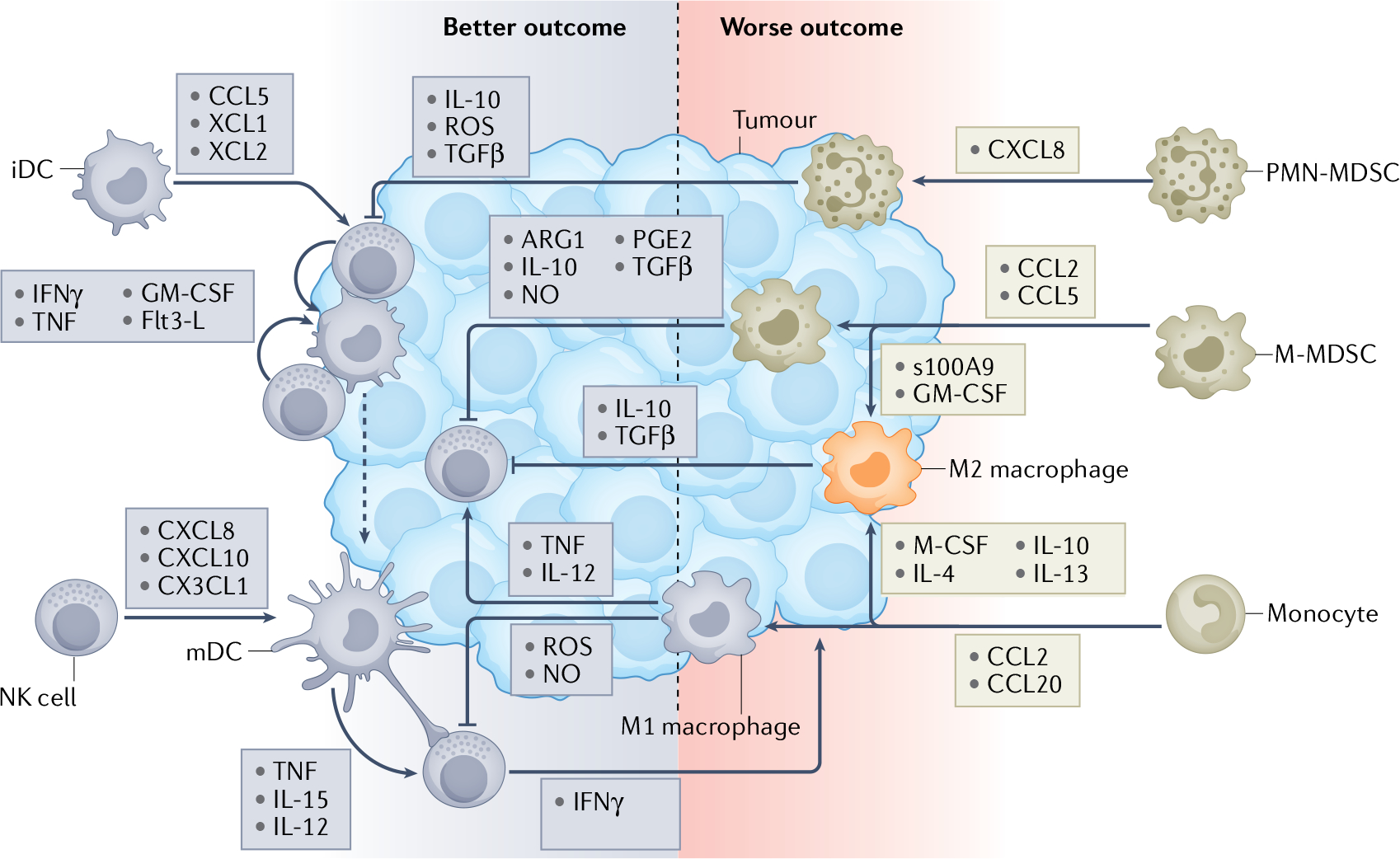
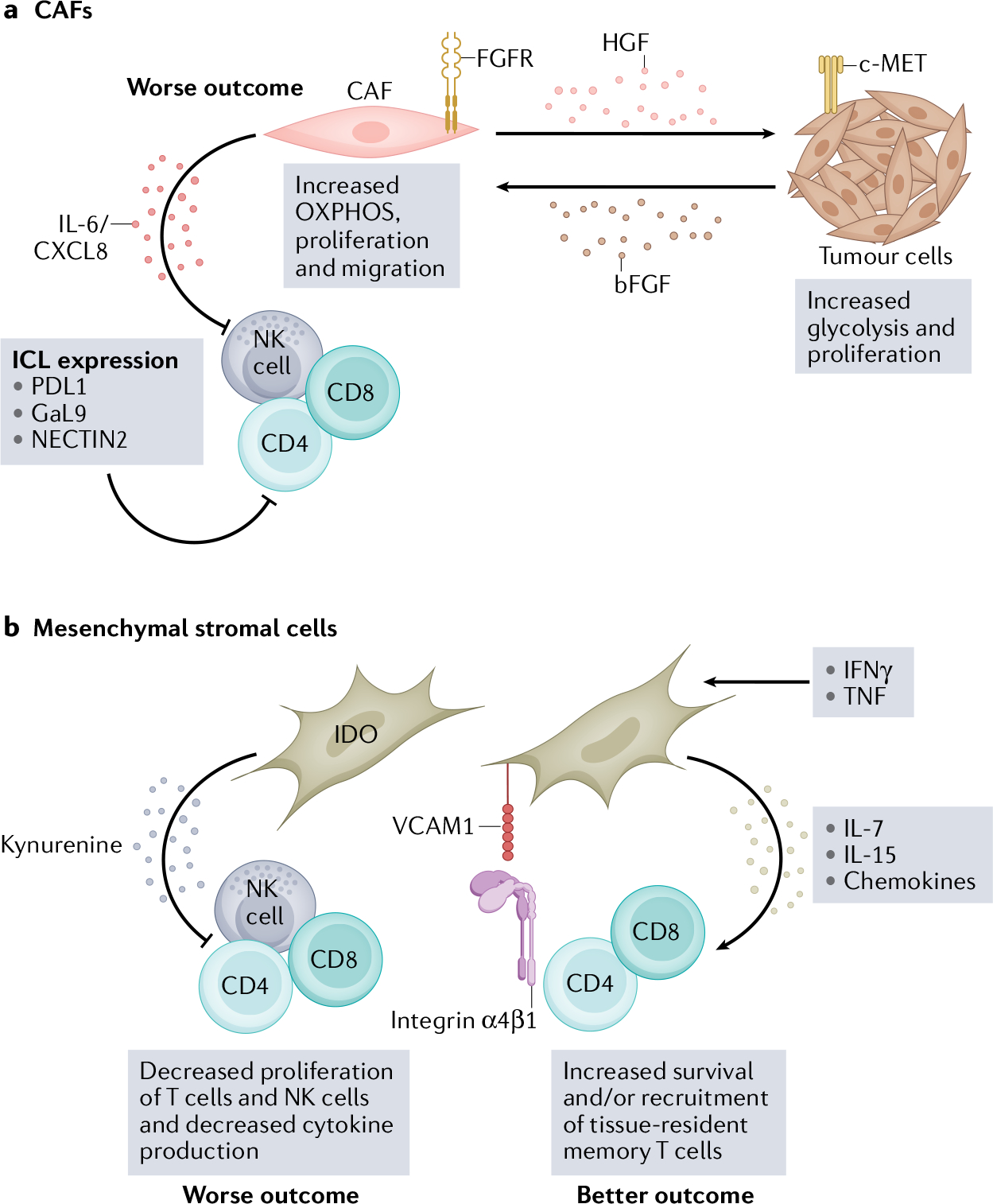
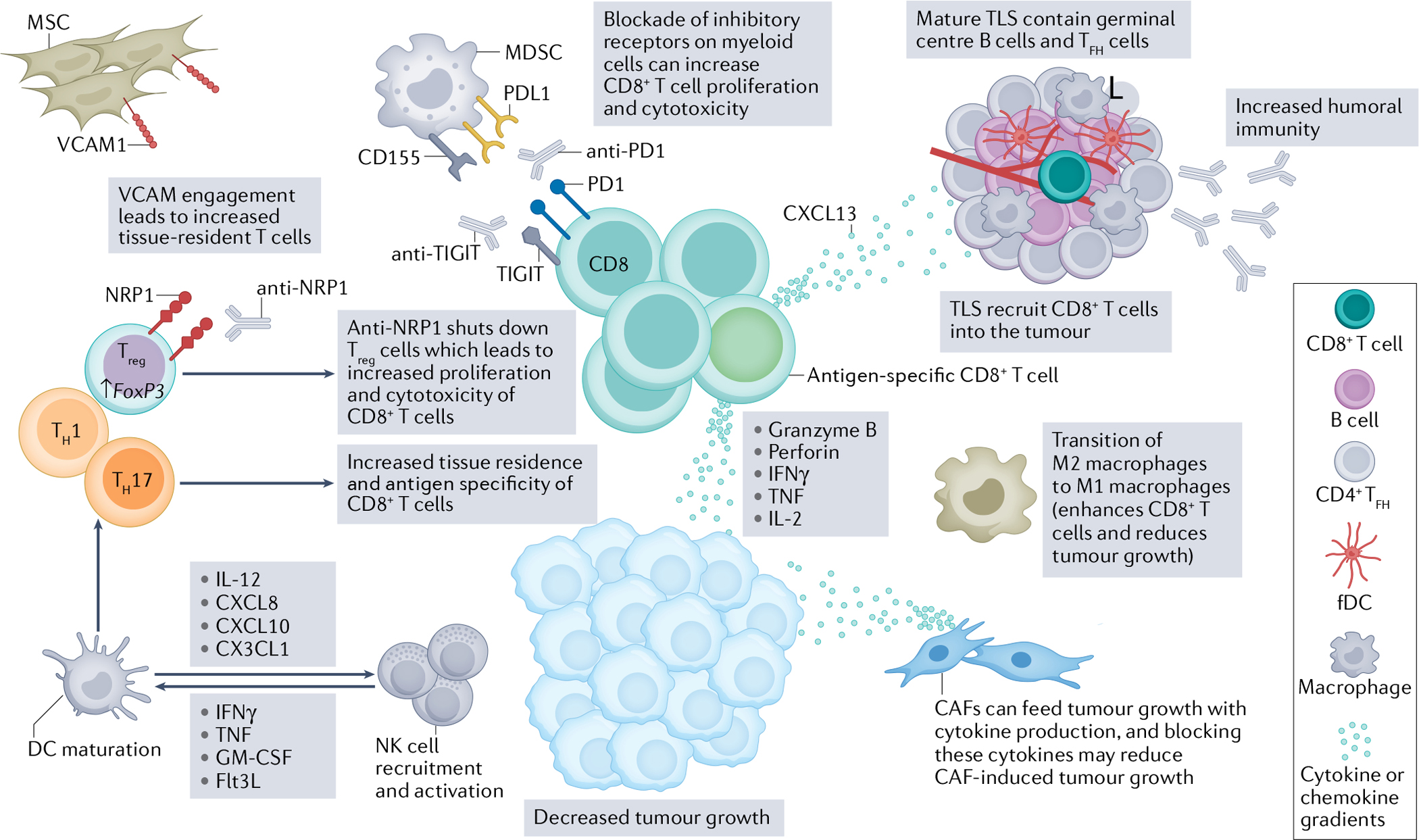
Targeted immunotherapy has improved patient survival in head and neck squamous cell carcinoma (HNSCC), but less than 20% of patients produce a durable response to these treatments. Thus, new immunotherapies that consider all key players of the complex HNSCC tumour microenvironment (TME) are necessary to further enhance tumour-specific T cell responses in patients. HNSCC is an ideal tumour type in which to evaluate immune and non-immune cell differences because of two distinct TME aetiologies (human papillomavirus (HPV)-positive and HPV-negative disease), multiple anatomic sites for tumour growth, and clear distinctions between patients with locally advanced disease and those with recurrent and/or metastatic disease. Recent technological and scientific advancements have provided a more complete picture of all cellular constituents within this complex TME and have evaluated the interplay of both immune and non-immune cells within HNSCC. Here, we include a comprehensive analysis of the complete ecosystem of the HNSCC TME, performed utilizing data-rich resources such as The Cancer Genome Atlas, and cutting-edge techniques, such as single-cell RNA sequencing, high-dimensional flow cytometry and spatial multispectral imaging, to generate improved treatment strategies for this diverse disease.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests
L.V. is a co-inventor of a methodology licensed to INmune Bio, Inc., where soluble TNF sequestration using DN-TNF can be used to prevent or treat malignancies. D.P.Z. declares competing interests with Blueprint Medicines (advisory board), Macrogenics (consulting), Prelude Therapeutics (advisory board), and Merck (advisory board) and research support (institutional) from Merck, BMS, AstraZeneca, GlaxoSmithKline, Aduro, Astellas, Macrogenics, Lilly, Bicara, Checkmate Pharma, and Novasenta. R.L.F. declares competing interests with Aduro Biotech, Inc. (consulting), AstraZeneca/MedImmune (clinical trial, research funding), Bristol-Myers Squibb (advisory board, clinical trial, research funding), EMD Serono (advisory board), MacroGenics Inc. (advisory board), Merck (advisory board, clinical trial), Novasenta (consulting, stock, research funding), Numab Therapeutics AG (advisory board), Pfizer (advisory board), Sanofi (consultant), Tesaro (research funding) and Zymeworks Inc. (consultant). T.C.B. declares competing interests with Walking Fish Therapeutics (Scientific Advisory Board). The other authors declare no competing interests.
Figures
References
-
- Ferlay J et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 144, 1941–1953 (2019). - PubMed
-
- Sung H et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249 (2021). - PubMed
-
- HHS.gov. Smoking Cessation: A Report of the Surgeon General — Key Findings https://www.hhs.gov/surgeongeneral/reports-and-publications/tobacco/2020... (2020).
-
- Bray F et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68, 394–424 (2018). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
