

Differential roles of Aβ42/40, p-tau231 and p-tau217 for Alzheimer's trial selection and disease monitoring
- PMID: 36456833
- PMCID: PMC9800279
- DOI: 10.1038/s41591-022-02074-w
Differential roles of Aβ42/40, p-tau231 and p-tau217 for Alzheimer's trial selection and disease monitoring
Abstract
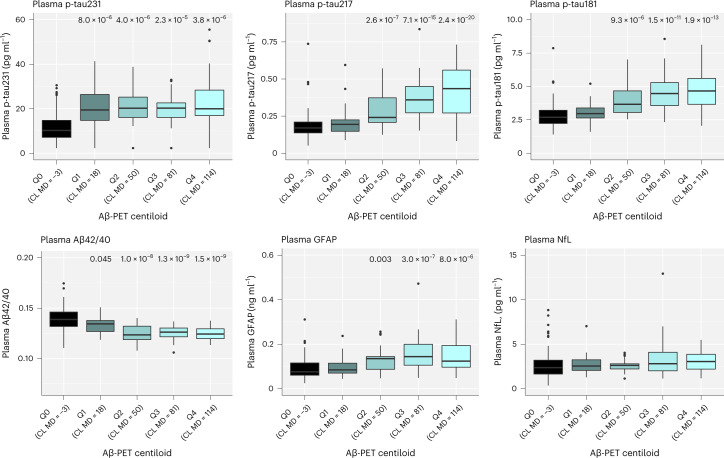
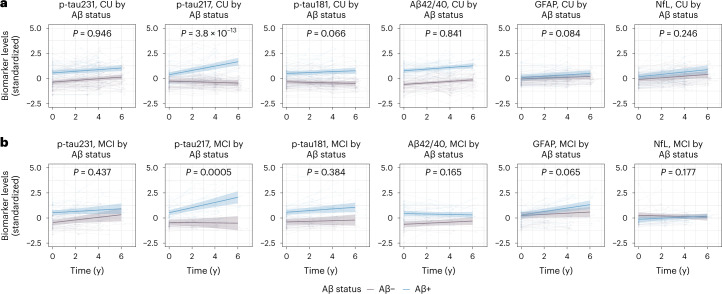
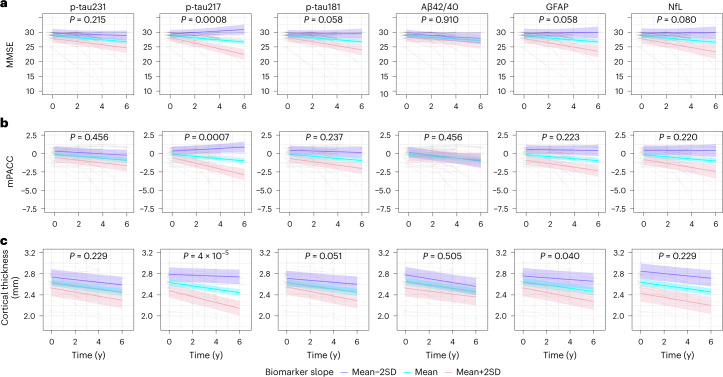
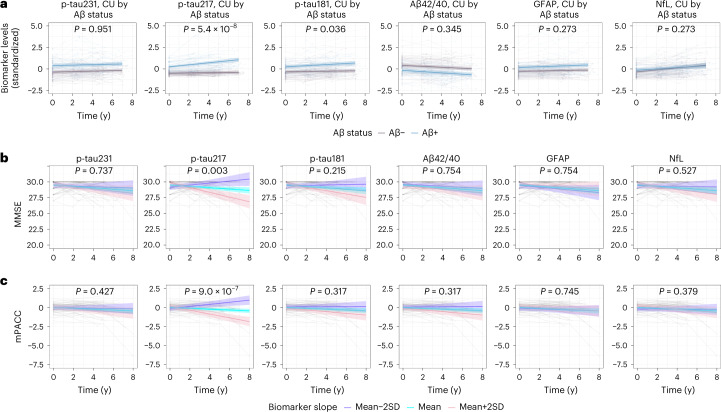
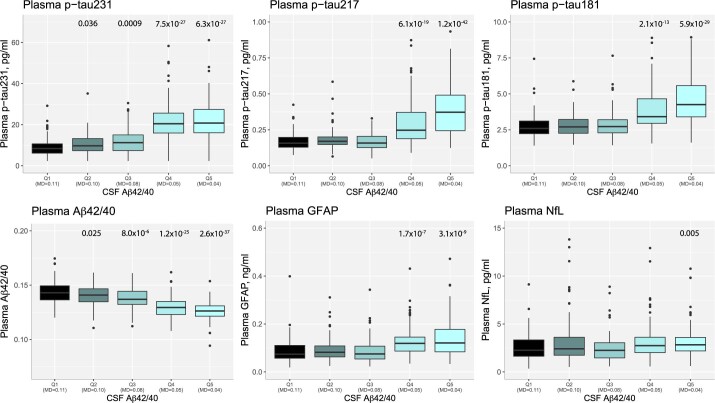
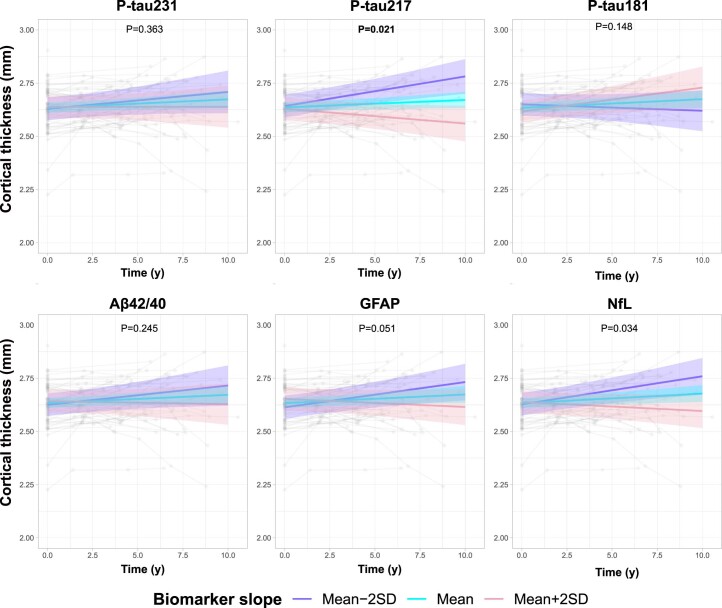
Blood biomarkers indicative of Alzheimer's disease (AD) pathology are altered in both preclinical and symptomatic stages of the disease. Distinctive biomarkers may be optimal for the identification of AD pathology or monitoring of disease progression. Blood biomarkers that correlate with changes in cognition and atrophy during the course of the disease could be used in clinical trials to identify successful interventions and thereby accelerate the development of efficient therapies. When disease-modifying treatments become approved for use, efficient blood-based biomarkers might also inform on treatment implementation and management in clinical practice. In the BioFINDER-1 cohort, plasma phosphorylated (p)-tau231 and amyloid-β42/40 ratio were more changed at lower thresholds of amyloid pathology. Longitudinally, however, only p-tau217 demonstrated marked amyloid-dependent changes over 4-6 years in both preclinical and symptomatic stages of the disease, with no such changes observed in p-tau231, p-tau181, amyloid-β42/40, glial acidic fibrillary protein or neurofilament light. Only longitudinal increases of p-tau217 were also associated with clinical deterioration and brain atrophy in preclinical AD. The selective longitudinal increase of p-tau217 and its associations with cognitive decline and atrophy was confirmed in an independent cohort (Wisconsin Registry for Alzheimer's Prevention). These findings support the differential association of plasma biomarkers with disease development and strongly highlight p-tau217 as a surrogate marker of disease progression in preclinical and prodromal AD, with impact for the development of new disease-modifying treatments.
© 2022. The Author(s).
Conflict of interest statement
N.J.A. has given lectures in symposia sponsored by Eli Lilly. S.J. has no disclosures. N.M.-C. has no disclosures. A.P.B. has no disclosures. O.S. has no disclosures. W.S.B. has no disclosures. T.K.K. has no disclosures. F.G.-O. has no disclosures. G.D.M. has no disclosures. F.J.M. has no disclosures. E.M.J. has no disclosures. R.L.K. has no disclosures. K.C. has no disclosures. T.J.B. has no disclosures. Y.L. has no disclosures. E.V. is a cofounder of ADx Neurosciences. S.P. has served on scientific advisory boards and/or given lectures in symposia sponsored by Biogen, Eli Lilly, Geras Solutions and Roche. E.S. has no disclosures. R.J.B. has equity ownership interest in C2N Diagnostics and may receive income based on technology licensed or optioned by Washington University to C2N Diagnostics, receives income from C2N Diagnostics for serving on the scientific advisory board and has received honoraria as a speaker/consultant/advisory board member from Amgen, Eisai and Roche. H.Z. has served at scientific advisory boards and/or as a consultant for Abbvie, Alector, Eisai, Denali, Roche Diagnostics, Wave, Samumed, Siemens Healthineers, Pinteon Therapeutics, Nervgen, AZTherapies, CogRx and Red Abbey Labs, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure and Biogen, and is a cofounder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work). S.C.J. has within the past 3 years served at scientific advisory boards and/or as a consultant for Roche Diagnostics, Prothena and Eisai and has received research support from Cerveau Technologies. K.B. has served as a consultant, at advisory boards, or at data monitoring committees for Abcam, Axon, BioArctic, Biogen, JOMDD/Shimadzu. Julius Clinical, Lilly, MagQu, Novartis, Ono Pharma, Pharmatrophix, Prothena, Roche Diagnostics and Siemens Healthineers, and is a cofounder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program, outside the work presented in this paper. O.H. has acquired research support (for the institution) from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer and Roche. In the past 2 years, he has received consultancy/speaker fees from Amylyx, Alzpath, BioArctic, Biogen, Cerveau, Fujirebio, Genentech, Novartis, Roche and Siemens.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
