

Differences between complex epithelial neoplasms of the ovary and high-grade serous ovarian cancer: a retrospective observational cohort study
- PMID: 36456989
- PMCID: PMC9714251
- DOI: 10.1186/s13048-022-01063-4
Differences between complex epithelial neoplasms of the ovary and high-grade serous ovarian cancer: a retrospective observational cohort study
Abstract
Background: Complex epithelial neoplasms of the ovary (CENO), an uncommon pathological histotype in ovarian cancer, comprises adenosquamous carcinoma and adenocarcinoma with metaplasia. Owing to the rarity of relevant reports, there are currently no statistics on outcomes based on large samples. Meanwhile high-grade serous ovarian cancer (HGSOC) is the most common histotype in ovarian cancer which has a recognized first-line treatment regimen and poor prognosis. Thus, we aimed to determine the characteristics, prognosis, and independent predictors of survival for CENO, compare them with those of HGSOC and construct prognostic predictive models and nomograms.
Methods: We used the Surveillance, Epidemiology, and End Results (SEER) database to determine patients diagnosed with CENO or HGSOC from 2000 to 2017. Clinical, demographic, and treatment characteristics were compared between these groups. Propensity score matching, Cox risk regression analysis, Kaplan-Meier survival curves, and the Least Absolute Shrinkage and Selection Operator regression analysis were employed for analyzing the data.
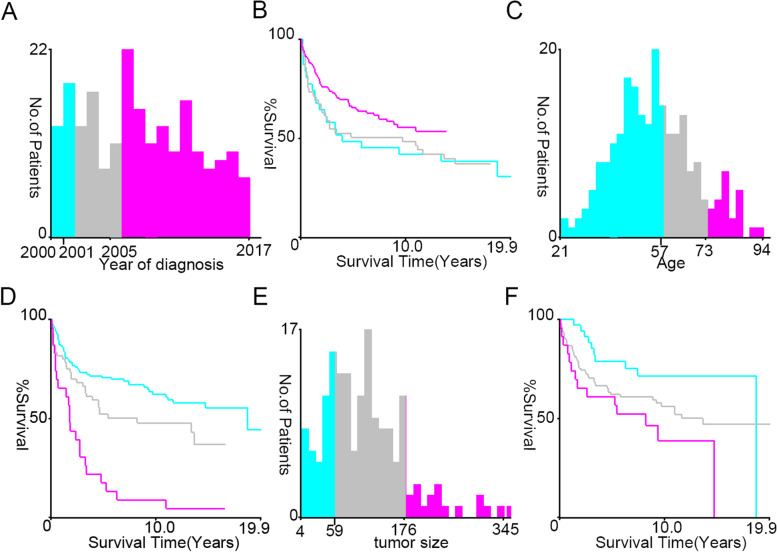
Results: Here, 31,567 patients with HGSOC and 216 patients with CENO between 2000 and 2017 in the SEER database were enrolled. Age < 57 years, unmarried, and early-stage diseases were more common in patients with CENO than in those with HGSOC. Women with CENO were less likely to receive adjuvant chemotherapy (65.7% vs. 79.4%) but more likely to receive radiotherapy (6.0% vs. 0.8%; both p < 0.001) than those with HGSOC. Year of diagnosis, surgery status, number of primary tumors, grade, and FIGO stage were independent prognostic factors for overall and cancer-specific survival in CENO. Overall survival rates were significantly lower for CENO than for more malignant HGSOC.
Conclusions: In summary, CENO was rare in ovarian cancer, while the year of diagnosis, surgery status, number of primary tumors, grade, and FIGO stage were independent prognostic factors. Compared with other common malignant ovarian tumors, CENO had a poor prognosis. Prognostic predictive models and nomograms had been determined to predict the individual survival rates of patients with CENO. These methods could improve evaluations of survival and therapeutic decisions for patients.
Keywords: Adenocarcinoma with metaplasia; Adenosquamous carcinoma; Cancer-specific survival; Complex epithelial neoplasms of the ovary; High-grade serous ovarian cancer; Overall survival; Propensity score matching; SEER database.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






References
-
- Meinhold-Heerlein I, Fotopoulou C, Harter P, Kurzeder C, Mustea A, Wimberger P, Hauptmann S, Sehouli J. The new WHO classification of ovarian, fallopian tube, and primary peritoneal cancer and its clinical implications. Arch Gynecol Obstet. 2016;293(4):695–700. doi: 10.1007/s00404-016-4035-8. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
