

Integrated clinical case discussions - a fully student-organized peer-teaching program on internal medicine
- PMID: 36457088
- PMCID: PMC9713160
- DOI: 10.1186/s12909-022-03889-4
Integrated clinical case discussions - a fully student-organized peer-teaching program on internal medicine
Abstract
Background: In response to students´ poor ratings of emergency remote lectures in internal medicine, a team of undergraduate medical students initiated a series of voluntary peer-moderated clinical case discussions. This study aims to describe the student-led effort to develop peer-moderated clinical case discussions focused on training cognitive clinical skill for first and second-year clinical students.
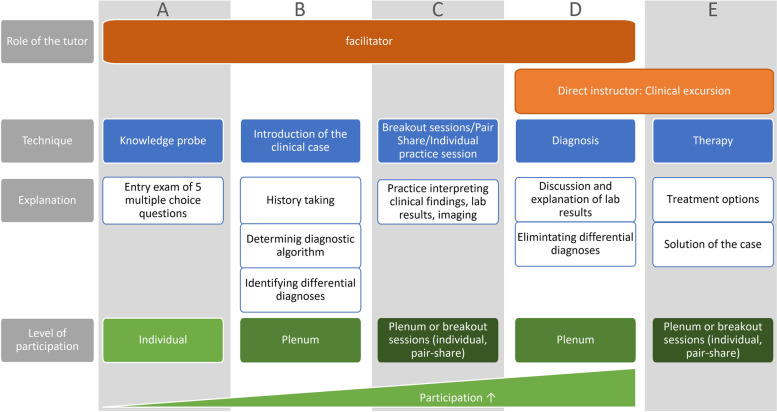
Methods: Following the Kern Cycle a didactic concept is conceived by matching cognitive learning theory to the competence levels of the German Medical Training Framework. A 50-item survey is developed based on previous evaluation tools and administered after each tutorial. Educational environment, cognitive congruence, and learning outcomes are assessed using pre-post-self-reports in a single-institution study.
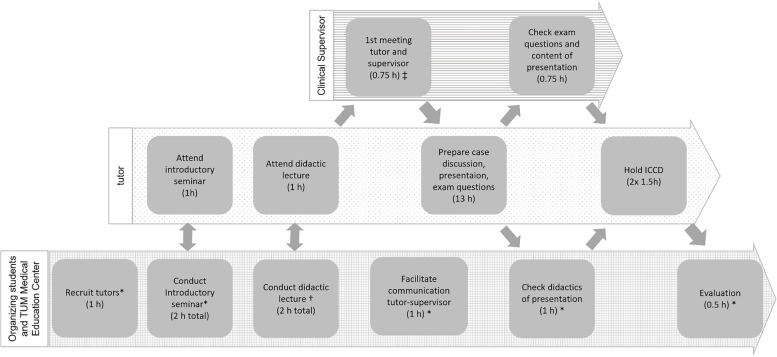
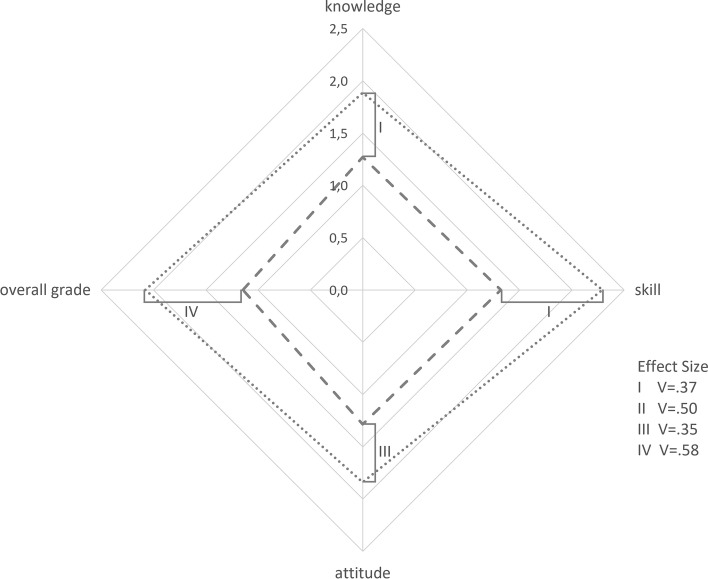
Results: Over the course of two semesters 19 tutors conducted 48 tutorials. There were 794 attendances in total (273 in the first semester and 521 in the second). The response rate was 32%. The didactic concept proved successful in attaining all learning objectives. Students rated the educational environment, cognitive congruence, and tutorials overall as "very good" and significantly better than the corresponding lecture. Students reported a 70%-increase in positive feelings about being tutored by peers after the session.
Conclusion: Peer-assisted learning can improve students´ subjective satisfaction levels and successfully foster clinical reasoning skills. This highlights successful student contributions to the development of curricula.
Keywords: Clinical Skills; Instructional Design; Peer-to-Peer; Problem-based/Clinical Case Discussion; Undergraduate Medical Education.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Seifman MA, Fuzzard SK, To H, Nestel D. COVID-19 impact on junior doctor education and training: a scoping review. Postgraduate Medical Journal. 2021:postgradmedj-2020–139575. doi:10.1136/postgradmedj-2020-139575 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
