

A plea for personalization of the hemodynamic management of septic shock
- PMID: 36457089
- PMCID: PMC9714237
- DOI: 10.1186/s13054-022-04255-y
A plea for personalization of the hemodynamic management of septic shock
Abstract
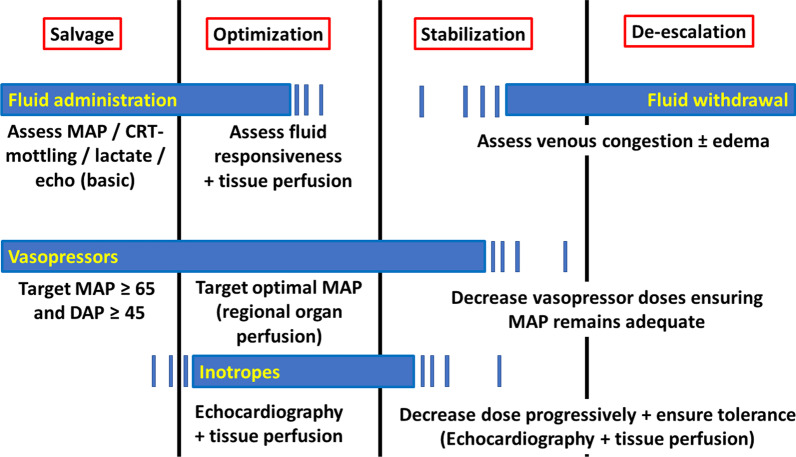
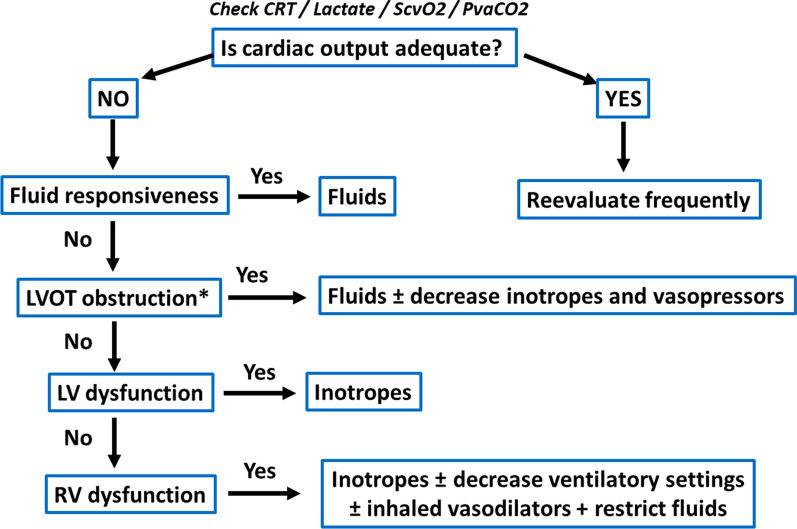
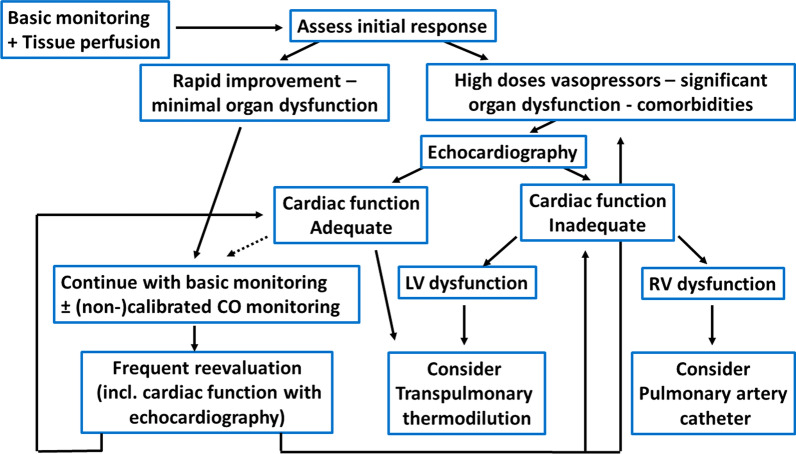
Although guidelines provide excellent expert guidance for managing patients with septic shock, they leave room for personalization according to patients' condition. Hemodynamic monitoring depends on the evolution phase: salvage, optimization, stabilization, and de-escalation. Initially during the salvage phase, monitoring to identify shock etiology and severity should include arterial pressure and lactate measurements together with clinical examination, particularly skin mottling and capillary refill time. Low diastolic blood pressure may trigger vasopressor initiation. At this stage, echocardiography may be useful to identify significant cardiac dysfunction. During the optimization phase, echocardiographic monitoring should be pursued and completed by the assessment of tissue perfusion through central or mixed-venous oxygen saturation, lactate, and carbon dioxide veno-arterial gradient. Transpulmonary thermodilution and the pulmonary artery catheter should be considered in the most severe patients. Fluid therapy also depends on shock phases. While administered liberally during the resuscitation phase, fluid responsiveness should be assessed during the optimization phase. During stabilization, fluid infusion should be minimized. In the de-escalation phase, safe fluid withdrawal could be achieved by ensuring tissue perfusion is preserved. Norepinephrine is recommended as first-line vasopressor therapy, while vasopressin may be preferred in some patients. Essential questions remain regarding optimal vasopressor selection, combination therapy, and the most effective and safest escalation. Serum renin and the angiotensin I/II ratio may identify patients who benefit most from angiotensin II. The optimal therapeutic strategy for shock requiring high-dose vasopressors is scant. In all cases, vasopressor therapy should be individualized, based on clinical evaluation and blood flow measurements to avoid excessive vasoconstriction. Inotropes should be considered in patients with decreased cardiac contractility associated with impaired tissue perfusion. Based on pharmacologic properties, we suggest as the first test a limited dose of dobutamine, to add enoximone or milrinone in the second line and substitute or add levosimendan if inefficient. Regarding adjunctive therapies, while hydrocortisone is nowadays advised in patients receiving high doses of vasopressors, patients responding to corticosteroids may be identified in the future by the analysis of selected cytokines or specific transcriptomic endotypes. To conclude, although some general rules apply for shock management, a personalized approach should be considered for hemodynamic monitoring and support.
Keywords: Blood pressure; Cardiac output; Fluids; Inotropic agents; Tissue perfusion; Vasopressor agents.
© 2022. The Author(s).
Conflict of interest statement
Daniel De Backer: Edwards Lifesciences, Philips, Baxter. Maurizio Cecconi: Edwards Lifesciences, Directed Systems. Michelle S Chew: Edwards Lifesciences. Ludhmila Hajjar No conflict of interest. Xavier Monnet: Gettinge. Gustavo Ospina-Tascon: No conflict of interest. Marlies Ostermann: Fresenius Medical, Baxter, Biomerieux. Michael R. Pinsky: Edwards LifeSciences, Baxter, Intelomed, Exostat. Jean-Louis Vincent: No conflict of interest.
Figures
References
-
- Cecconi M, De Backer D, Antonelli M, Beale RJ, Bakker J, Hofer C, Jaeschke R, Mebazaa A, Pinsky MR, Teboul JL, et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40(12):1795–1815. doi: 10.1007/s00134-014-3525-z. - DOI - PMC - PubMed
-
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, Machado FR, McIntyre L, Ostermann M, Prescott HC, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi: 10.1007/s00134-021-06506-y. - DOI - PMC - PubMed
-
- Coopersmith CM, De Backer D, Deutschman CS, Ferrer R, Lat I, Machado FR, Martin GS, Martin-Loeches I, Nunnally ME, Antonelli M, et al. Surviving sepsis campaign: research priorities for sepsis and septic shock. Intensive Care Med. 2018;44(9):1400–1426. doi: 10.1007/s00134-018-5175-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
