

doi: 10.1016/j.eats.2022.07.018.
eCollection 2022 Nov.
Low-Flow Ankle Arthroscopy for Gunshot Wounds With Retained Intra-Articular Ballistic
Affiliations
- PMID: 36457388
- PMCID: PMC9705770
- DOI: 10.1016/j.eats.2022.07.018
Item in Clipboard
Low-Flow Ankle Arthroscopy for Gunshot Wounds With Retained Intra-Articular Ballistic
Arthrosc Tech.
.
Abstract
Gunshot injuries to the foot and ankle can cause unique and challenging situations for orthopaedic surgeons. The foot and ankle have limited soft-tissue coverage and highly congruent joint spaces, leading to injuries that are often intra-articular with substantial tissue loss. These injuries are often confounded by feet shod in footwear that is pulled into the path of the missile and corresponding tissue. Thus, we report our experience of using low-flow arthroscopy for extraction of retained ballistics, while irrigating and debriding the path of the missile.
© 2022 The Authors.
Figures

(A-D) Anteroposterior (AP) and lateral radiographs and associated coronal and sagittal computed tomography (CT) images of the ankle demonstrating evidence of an intra-articular ballistic missile with underlying talar neck fracture. Intra-articular ballistic foreign bodies are appreciated within the ankle and subtalar joints. (E-H) AP and lateral radiographs and associated coronal and sagittal CT images of the ankle demonstrating evidence of an intra-articular ballistic missile with underlying talar neck, talar body and medial malleolus fractures. (I-L) AP and lateral radiographs and associated sagittal CT images of the ankle demonstrating evidence of an intra-articular ballistic missile with underlying posterior talar body and posterior malleolus fractures.
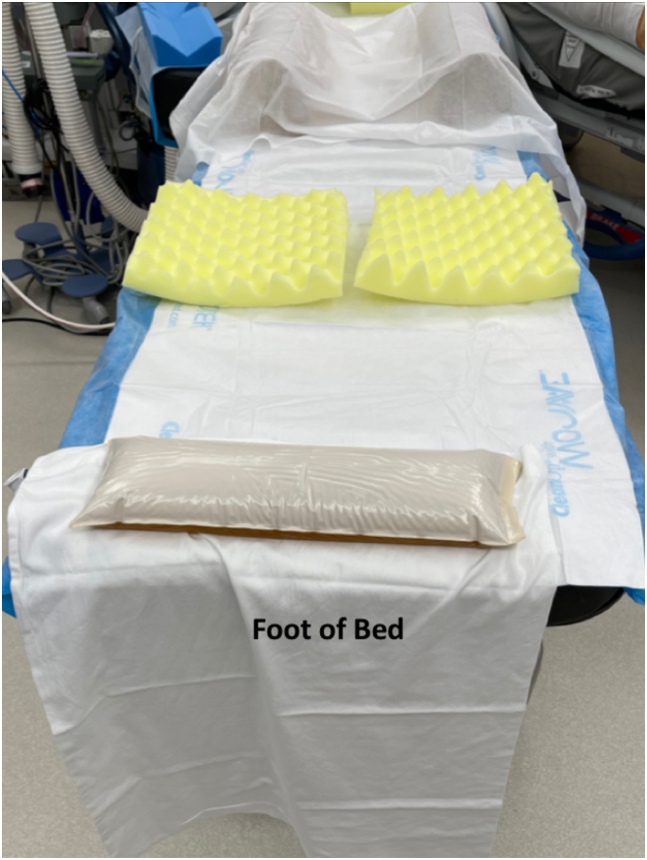
Operative table setup for completion of prone ankle arthroscopic procedures demonstrating 2 gel foam bumps positioned underneath the patient’s shoulders, foam padding for the patient’s knees, and a small gel foam bump for positioning of the ankle. Gel foam bumps and foam padding is placed to ensure all boney prominences are well padded. The gel foam bump at the end of the table allows for the ankle to be manipulated during the course of the procedure.

Before initiating a prone ankle arthroscopy, pertinent anatomical structures are marked, including the borders of the medial and lateral malleolus, edges of the calcaneal tuberosity, medial and lateral edge of the Achilles tendon, and path of the sural nerve. When being viewed from the lateral side, the borders of the fibula (F), approximate course of the sural nerve (S), and borders of the Achilles tendon should be marked to determine appropriate portal placement.

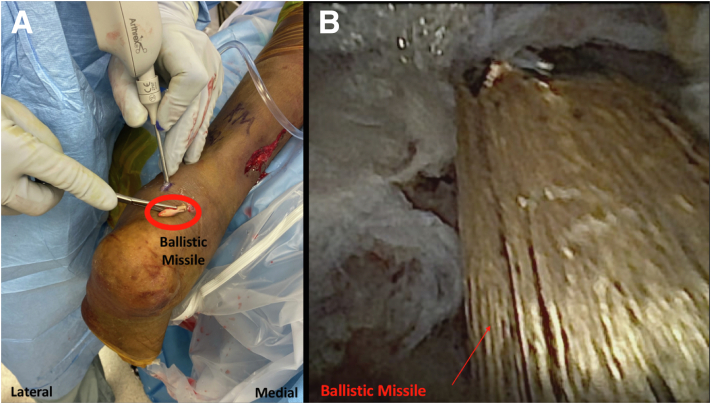
This particular patient was positioned prone for completion of the procedure based on the location of their intra-articular ballistic fragment. The standard nick-and-spread technique is used for creation of each portal on the medial and lateral side of the Achilles tendon. (A) The NanoScope (Arthrex, Naples FL) is inserted within the posteromedial portal for complete visualization of the ankle joint. A probe can be visualized within the posterolateral portal, which is used to evaluate intra-articular structures arthroscopically. (B) Arthroscopic view from the posteromedial portal demonstrating evidence of intra-articular talus fracture involving the subtalar joint. An arthroscopic shaver is placed within the posterolateral portal to debride loose osteochondral fragments and hemorrhagic tissue.
This patient is positioned prone for completion of the procedure based on the location of their intra-articular ballistic fragment. (A) The NanoScope (Arthrex, Naples FL) is shown within the posteromedial portal. The intra-articular projectile was removed successfully from the ankle joint using a retriever with the tip pointed toward the posterolateral portal. The projectile is shown outside of the patient’s ankle. The NanoScope (Arthrex) is then used to perform irrigation and debridement of the path of the missile. (B) Intra-articular ballistic missile being extracted from the joint space with the tip facing the portal entry site.
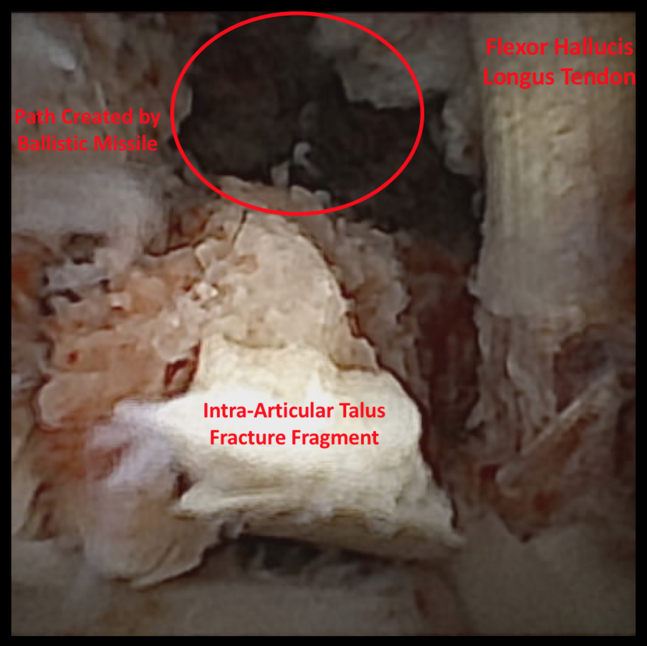
Arthroscopic view of the ankle from the posterolateral portal after extraction of the intra-articular ballistic missile. The flexor hallucis tendon can be viewed just medial to the path created by the projectile. Intra-articular osteochondral fragments with surrounding hemorrhagic tissue can be appreciated.

This patient was positioned supine for completion of the procedure based on the location of their intra-articular ballistic fragment. While performing arthroscopic removal of the projectile, a large amount of bone loss was appreciated within the talar body. The residual bone loss is being addressed acutely with primary grafting with arthroscopically injectable putty through a standard anteromedial portal under direct visualization using the nanoscope within the anterolateral portal (Arthrex, Naples FL).

Mini C-arm fluoroscopic image of the lateral ankle demonstrating no evidence of any radio-opaque foreign bodies within the ankle joint after successful removal of the intra-articular ballistic missile using low-flow arthroscopy.
References
-
- Court-Brown C.M., Heckman J.D., McQueen M.M., et al. 8th ed. Wolters Kluwer Health; Philadelphia, PA: 2014. Rockwood and Green’s fractures in adults.
-
- Holmes G.B. Gunshot wounds of the foot. Clin Orthop Relat Res. 2003;408:86–91. - PubMed
-
- Knapp T.P., Patzakis M.J., Lee J., Seipel P.R., Abdollahi K., Reisch R.B. Comparison of intravenous and oral antibiotic therapy in the treatment of fractures caused by low-velocity gunshots: A prospective, randomized study of infection rates. J Bone Joint Surg Am. 1996;78:1167–1171. - PubMed
-
- Gonzalez T., Briceno J., Velaso B., et al. Gunshot-related injuries to the foot & ankle: Review article. Foot Ankle Int. 2020;41:486–496. - PubMed
-
- Bartlett C.S., Helfet D.L., Hausman M.R., Strauss E. Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg. 2000;8:21–36. - PubMed
LinkOut - more resources
Full Text Sources
