

Epidermal growth factor receptor mutations and brain metastases in non-small cell lung cancer
- PMID: 36457515
- PMCID: PMC9707620
- DOI: 10.3389/fonc.2022.912505
Epidermal growth factor receptor mutations and brain metastases in non-small cell lung cancer
Abstract
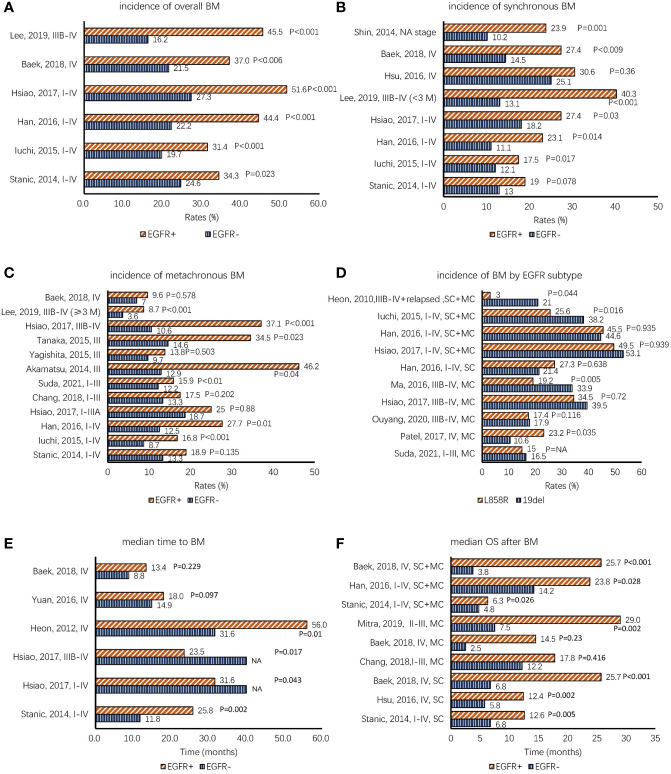
Studies have revealed that non-small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) mutations has a high incidence of brain metastases (BMs). However, the association between EGFR mutations and BMs remains unknown. This review summarizes detailed information about the incidence of BMs, clinical and imaging characteristics of BMs, brain surveillance strategies, influence of treatments on BMs, prognosis after BMs, and differences in EGFR mutations between paired primary tumors and BMs in EGFR-mutated NSCLC. The prognostic results demonstrate that patients with mutated EGFR have a higher incidence of BMs, EGFR tyrosine kinase inhibitors (EGFR-TKIs) (afatinib and osimertinib) delay the development of BMs, and patients with mutated EGFR with synchronous or early BMs have better overall survival after BMs than those with wild-type EGFR. The EGFR mutation status of BM sites is not always in accordance with the primary tumors, which indicates that there is heterogeneity in EGFR gene status between paired primary tumors and BMs. However, the EGFR gene status of the primary site can largely represent that of BM sites. Among patients developing synchronous BMs, patients with mutated EGFR are less likely to have central nervous system (CNS) symptoms than patients with wild-type EGFR. However, the possibility of neuro-symptoms is high in patients with metachronous BMs. Patients with mutated EGFR tend to have multiple BMs as compared to patients with wild-type EGFR. Regarding very early-stage NSCLC patients without neuro-symptoms, regular neuroimaging follow-up is not recommended. Among advanced NSCLC patients with EGFR mutation, liberal brain imaging follow-up in the first several years showed more advantages in terms of cost.
Keywords: EGFR mutation; brain metastasis; characteristics; genetic heterogeneity; non-small cell lung cancer; prognosis.
Copyright © 2022 Zhao, Zhou, Rong, Sun, Lin, Wang, Wang, Wang and Hui.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Heon S, Yeap BY, Britt GJ, Costa DB, Rabin MS, Jackman DM, et al. . Development of central nervous system metastases in patients with advanced non-small cell lung cancer and somatic egfr mutations treated with gefitinib or erlotinib. Clin Cancer rese: an Off J Am Assoc Cancer Res (2010) 16(23):5873–82. doi: 10.1158/1078-0432.CCR-10-1588 - DOI - PMC - PubMed
-
- Su PL, Wu YL, Chang WY, Ho CL, Tseng YL, Lai WW, et al. . Preventing and treating brain metastases with three first-line egfr-tyrosine kinase inhibitors in patients with egfr mutation-positive advanced non-small cell lung cancer. Ther Adv Med Oncol (2018) 10:1758835918797589. doi: 10.1177/1758835918797589 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous