

Perioperative chemotherapy in colorectal cancer with peritoneal metastases: A global propensity score matched study
- PMID: 36457647
- PMCID: PMC9706515
- DOI: 10.1016/j.eclinm.2022.101746
Perioperative chemotherapy in colorectal cancer with peritoneal metastases: A global propensity score matched study
Abstract
Background: There is a paucity of studies evaluating perioperative systemic chemotherapy in conjunction with cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) in patients with colorectal cancer peritoneal metastases (CRCPM). The aim was to evaluate neoadjuvant and/or adjuvant systemic therapy in CRCPM.
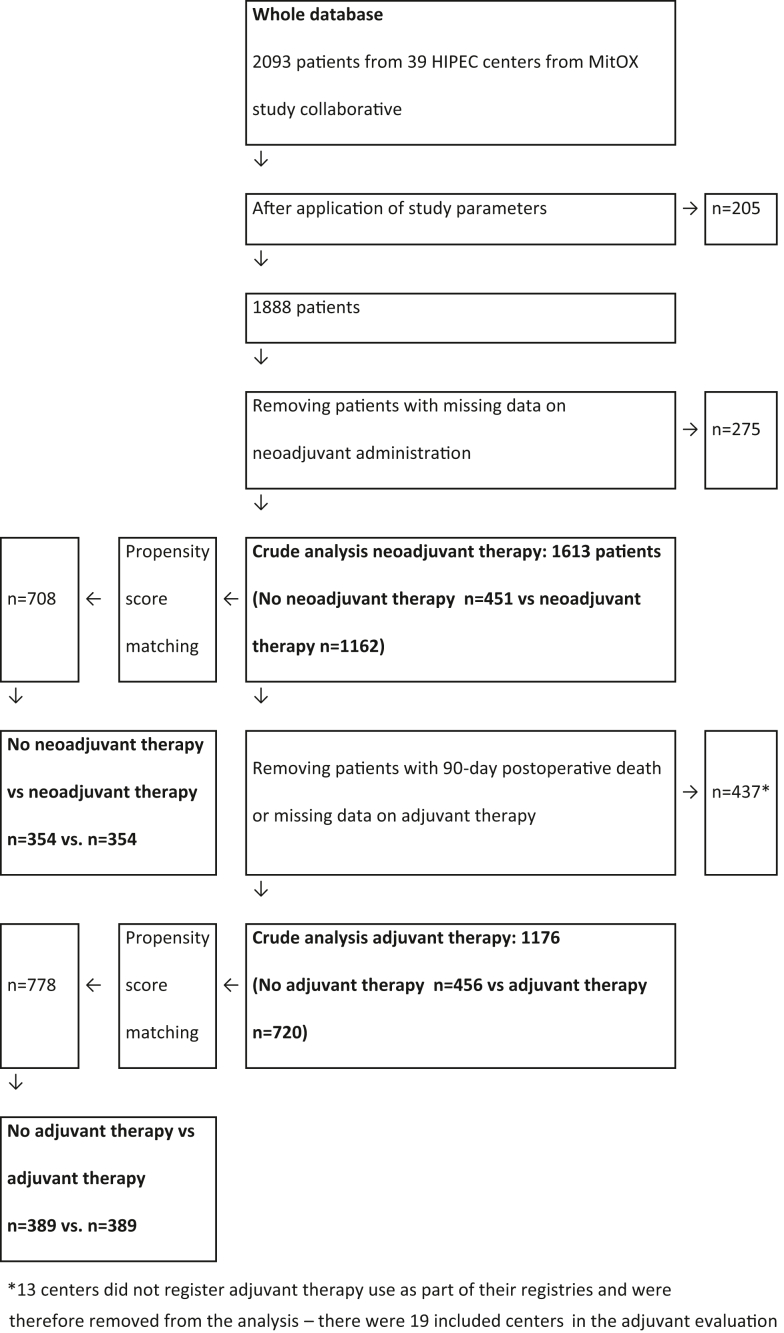
Methods: Patients with CRCPM from 39 treatment centres globally from January 1, 1991, to December 31, 2018, who underwent CRS+HIPEC were identified and stratified according to neoadjuvant/adjuvant use. Crude data analysis, propensity score matching (PSM) and Cox-proportional hazard modelling was performed.
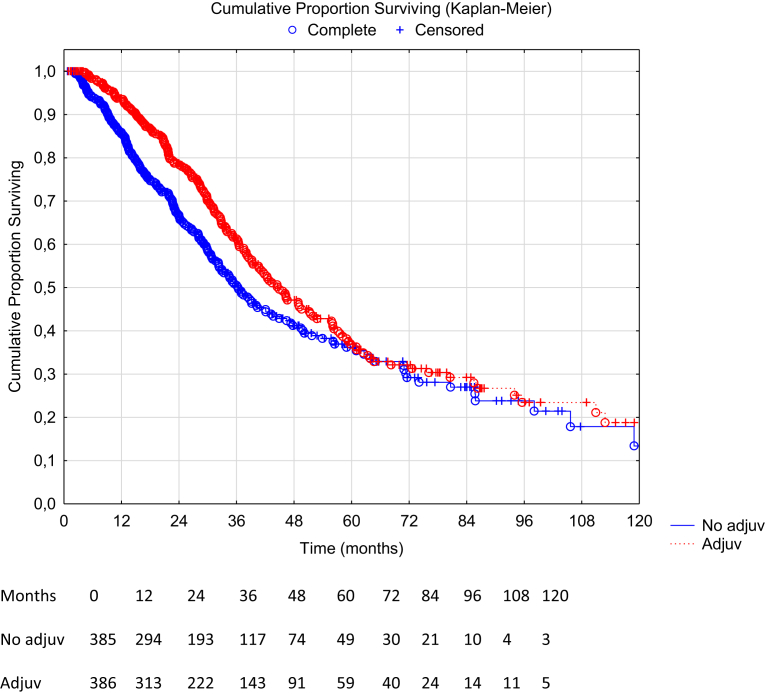
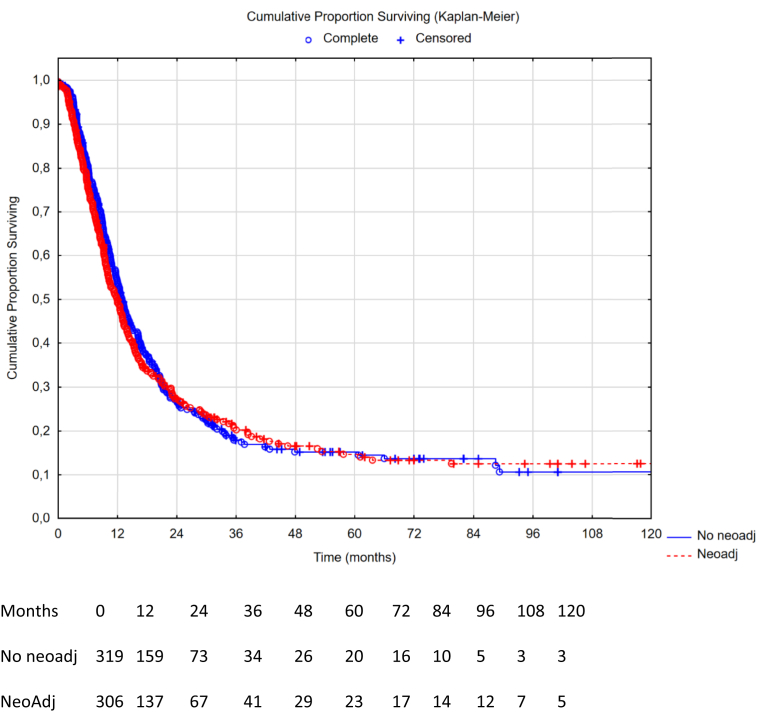
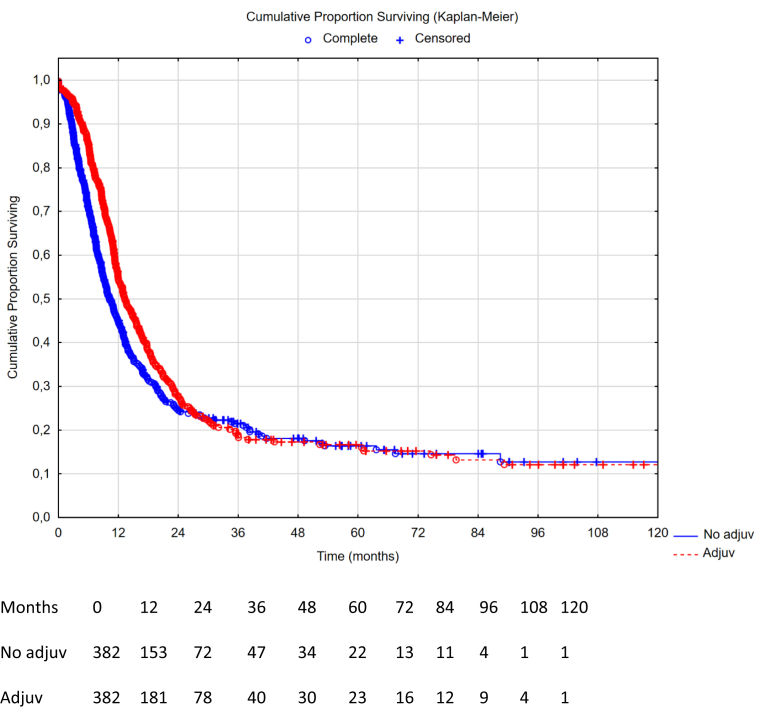
Findings: Of 2093 patients, 1613 were included in neoadjuvant crude evaluation with 708 in the PSM cohort (354 patients/arm). In the adjuvant evaluation, 1176 patients were included in the crude cohort with 778 in the PSM cohort (389 patients/arm). The median overall survival (OS) in the PSM cohort receiving no neoadjuvant vs neoadjuvant therapy was 37.0 months (95% CI: 32.6-42.7) vs 34.7 months (95% CI: 31.2-38.8, HR 1.08 95% CI: 0.88-1.32, p = 0.46). The median OS in the PSM cohort receiving no adjuvant therapy vs adjuvant therapy was 37.0 months (95% CI: 32.9-41.8) vs 45.7 months (95% CI: 38.8-56.2, HR 0.79 95% CI: 0.64-0.97, p = 0.022). Recurrence-free survival did not differ in the neoadjuvant evaluation but differed in the adjuvant evaluation - HR 1.04 (95% CI: 0.87-1.25, p = 0.66) and 0.83 (95% CI: 0.70-0.98, p = 0.03), respectively. Multivariable Cox-proportional hazard modelling in the crude cohorts showed hazard ratio 1.08 (95% CI: 0.92-1.26, p = 0.37) for administering neoadjuvant therapy and 0.86 (95% CI: 0.72-1.03, p = 0.095) for administering adjuvant therapy.
Interpretation: Neoadjuvant therapy did not confer a benefit to patients undergoing CRS+HIPEC for CRCPM, whereas adjuvant therapy was associated with a benefit in this retrospective setting.
Funding: None.
Keywords: Adjuvant chemotherapy; Colorectal cancer; Cytoreductive surgery; Hyperthermic intraperitoneal chemotherapy; Neoadjuvant chemotherapy; Peritoneal metastases.
© 2022 The Author(s).
Conflict of interest statement
Oliver M. Fisher reports personal fees from GORE and Fisher & Paykel Healthcare outside the submitted work. Olivier Glehen is consultant for GAMIDA.
Figures

References
-
- Franko J., Shi Q., Meyers J.P., et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomised trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) database. Lancet Oncol. 2016;17:1709–1719. - PubMed
-
- Quénet F., Elias D., Roca L., et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22:256–266. - PubMed
-
- Bushati M., Rovers K.P., Sommariva A., et al. The current practice of cytoreductive surgery and HIPEC for colorectal peritoneal metastases: results of a worldwide web-based survey of the Peritoneal Surface Oncology Group International (PSOGI) Eur J Surg Oncol. 2018;44:1942–1948. - PubMed
-
- Rovers K.P., Bakkers C., Simkens G.A.A.M., et al. Perioperative systemic therapy and cytoreductive surgery with HIPEC versus upfront cytoreductive surgery with HIPEC alone for isolated resectable colorectal peritoneal metastases: protocol of a multicentre, open-label, parallel-group, phase II-III, randomised, superiority study (CAIRO6) BMC Cancer. 2019;19:390. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
