

Clinical outcomes following discontinuation of renin-angiotensin-system inhibitors in patients with type 2 diabetes and advanced chronic kidney disease: A prospective cohort study
- PMID: 36457651
- PMCID: PMC9706514
- DOI: 10.1016/j.eclinm.2022.101751
Clinical outcomes following discontinuation of renin-angiotensin-system inhibitors in patients with type 2 diabetes and advanced chronic kidney disease: A prospective cohort study
Abstract
Background: Renin-angiotensin-system inhibitors (RASi), that include angiotensin converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) reduce proteinuria, delay chronic kidney disease (CKD) progression, protect against cardiovascular events and heart failure hospitalizations. We examined the associations of discontinuation of ACEi/ARBs with risk of clinical outcomes in Chinese patients with type 2 diabetes (T2D) and advanced-CKD (estimated-glomerular filtration rate [eGFR] <30 ml/min/1.73 m2).
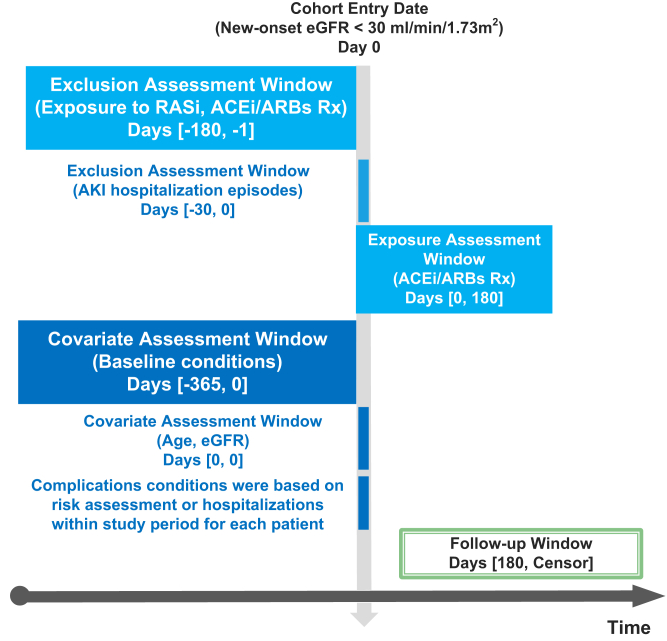
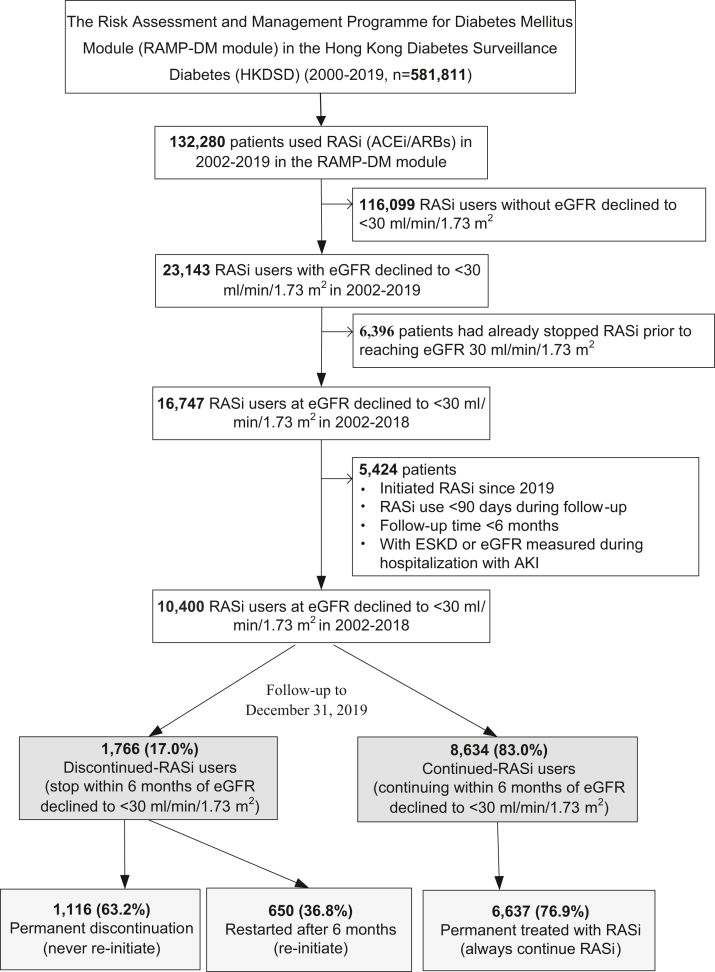
Methods: We conducted a prospective, population-based cohort study including 10,400 patients with T2D in Hong Kong stratified by continuation of ACEi/ARBs within 6 months after reaching eGFR <30 ml/min/1.73 m2 from January 01, 2002 to December 31, 2018 and observed until December 31, 2019. The primary outcomes were death, major-adverse cardiovascular events (MACE), heart failure, end-stage kidney disease (ESKD), and all-cause mortality. Cox-model with time-dependent exposure and covariates was used to estimate the hazard ratio (HR) of outcomes in a propensity-score overlap-weighted cohort. The risk of occurrence of hyperkalemia (plasma potassium >5.5 mmol/L) in discontinued-ACEi/ARBs versus continued-ACEi/ARBs users was assessed in a register-based cohort.
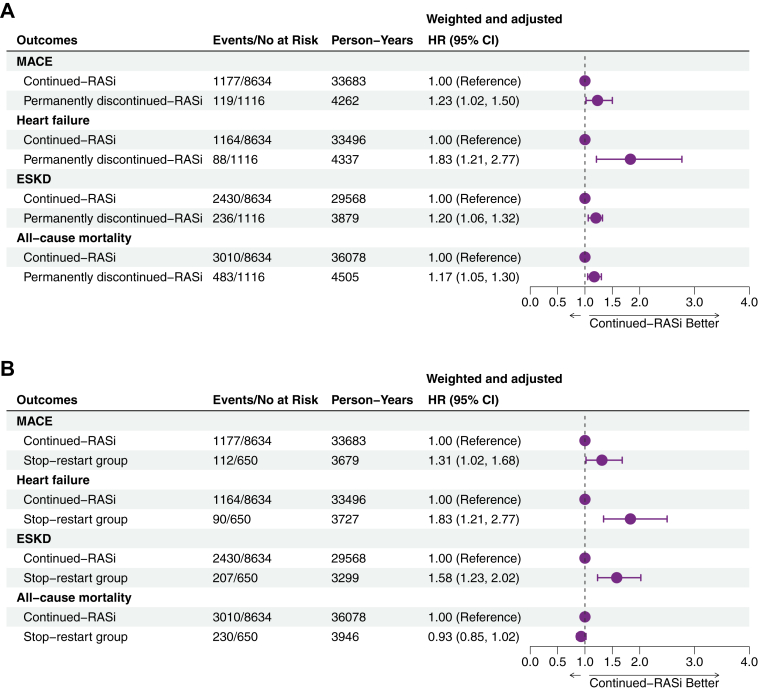
Findings: In the population-based cohort of 10,400 ACEi/ARBs users with new-onset eGFR<30 ml/min/1.73 m2, 1766 (17.0%) discontinued ACEi/ARBs and 8634 (83.0%) persisted with treatment. During a median follow-up of 3.6 (interquartile range, IQR: 2.11-5.8) years (41,623 person-years), 13.5%, 12.9%, and 27.6% had incident MACE, heart failure and ESKD respectively, and 35.8% died. Discontinued-ACEi/ARBs use was associated with higher risk of MACE (HR = 1.27, 95% CI: 1.08-1.49), heart failure (HR = 1.85, 95% CI: 1.53-2.25) and ESKD (HR = 1.30, 95% CI: 1.17-1.43), and neutral risk of all-cause mortality (HR = 0.93, 95% CI: 0.86-1.01) compared to counterparts with continued use. In the register-based cohort (583 discontinued-ACEi/ARBs users and 3817 continued-ACEi/ARBs users), discontinued-ACEi/ARBs had neutral risk of hyperkalemia (HR = 0.95, 95% CI: 0.84-1.08).
Interpretation: Discontinuation of ACEi/ARBs was associated with increased risk of cardiovascular-renal events supporting their continued use in patients with T2D and advanced-CKD.
Funding: CUHK Impact Research Fellowship Scheme.
Keywords: Angiotensin receptor antagonists; Angiotensin-converting enzyme inhibitors; Cardiovascular disease; Chronic kidney disease; Diabetes; Mortality; Therapeutics.
© 2022 The Author(s).
Conflict of interest statement
JCNC has received research grants and/or honoraria for consultancy or giving lectures, from 10.13039/100004325AstraZeneca, 10.13039/100004326Bayer, Boehringer Ingelheim, 10.13039/100004312Eli Lilly & Co, Hua Medicine, Lee Powder, Merck Serono, 10.13039/100009947Merck Sharp & Dohme, 10.13039/100004319Pfizer, 10.13039/501100011725Servier, 10.13039/100004339Sanofi and Viatris Pharmaceutical. APSK has received research grants and/or speaker honoraria from Abbott, 10.13039/100004325AstraZeneca, 10.13039/100004326Bayer, Boehringer Ingelheim, Eli-Lilly, Kyowa Kirin, Merck Serono, Nestle, 10.13039/501100004191Novo Nordisk, 10.13039/100004319Pfizer and 10.13039/100004339Sanofi. AOYL has served as a member of advisory panel for Amgen, AstraZeneca, Boehringer Ingelheim and Sanofi and received research support from Amgen, Asia Diabetes Foundation, Bayer, Boehringer Ingelheim, Lee's Pharmaceutical, MSD, Novo Nordisk, Roche, Sanofi, Sugardown Ltd, Takeda. None of these relationships had any influence on the content of the present manuscript. RCWM has received research funding from 10.13039/100004325AstraZeneca, 10.13039/100004326Bayer, Merck Sharp & Dohme, 10.13039/501100004191Novo Nordisk, 10.13039/100004319Pfizer and Tricida Inc. for carrying out clinical trials, and has received speaker honorarium or consultancy in advisory boards from AstraZeneca, Bayer and Kyowa Kirin. All proceeds have been donated to the Chinese University of Hong Kong to support diabetes research. Other authors have no conflicts of interest to disclose.
Figures

References
-
- Brenner B.M., Cooper M.E., De Zeeuw D., et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345(12):861–869. - PubMed
-
- Dagenais G.R., Yusuf S., Bourassa M.G., et al. Effects of ramipril on coronary events in high-risk persons. Circulation. 2001;104(5):522–526. - PubMed
-
- Lewis E.J., Hunsicker L.G., Clarke W.R., et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345(12):851–860. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
