

Development of artificial neural network models for paediatric critical illness in South Africa
- PMID: 36458145
- PMCID: PMC9705750
- DOI: 10.3389/fped.2022.1008840
Development of artificial neural network models for paediatric critical illness in South Africa
Abstract
Objectives: Failures in identification, resuscitation and appropriate referral have been identified as significant contributors to avoidable severity of illness and mortality in South African children. In this study, artificial neural network models were developed to predict a composite outcome of death before discharge from hospital or admission to the PICU. These models were compared to logistic regression and XGBoost models developed on the same data in cross-validation.
Design: Prospective, analytical cohort study.
Setting: A single centre tertiary hospital in South Africa providing acute paediatric services.
Patients: Children, under the age of 13 years presenting to the Paediatric Referral Area for acute consultations.
Outcomes: Predictive models for a composite outcome of death before discharge from hospital or admission to the PICU.
Interventions: None.
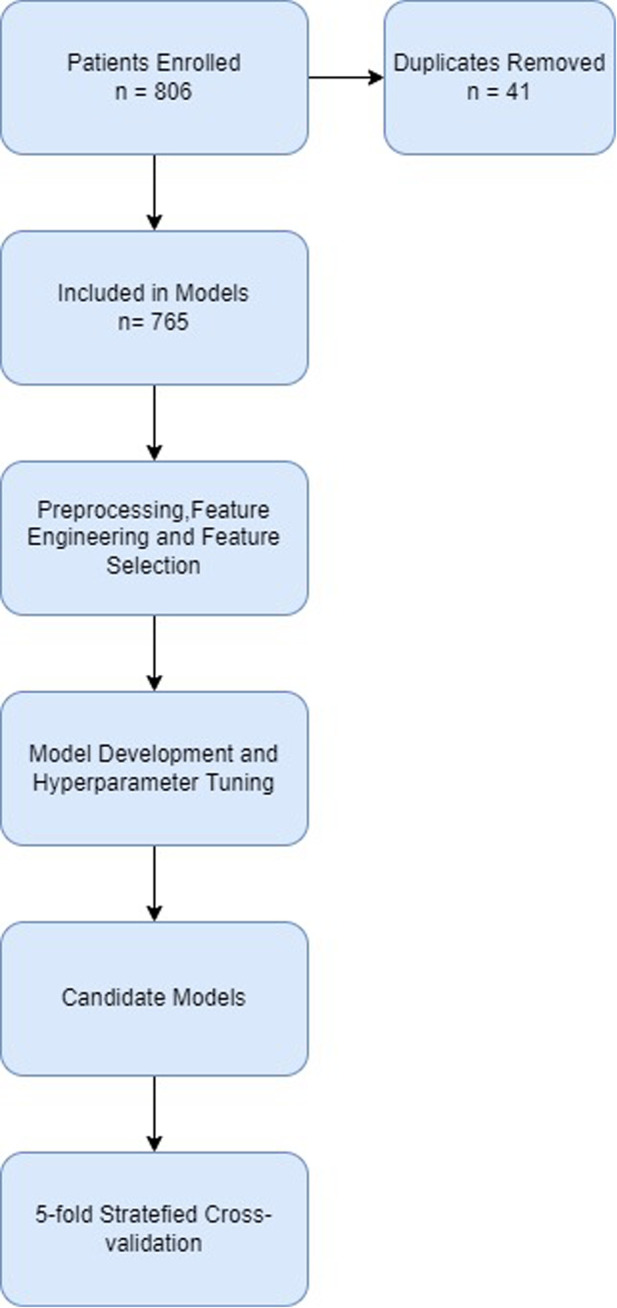
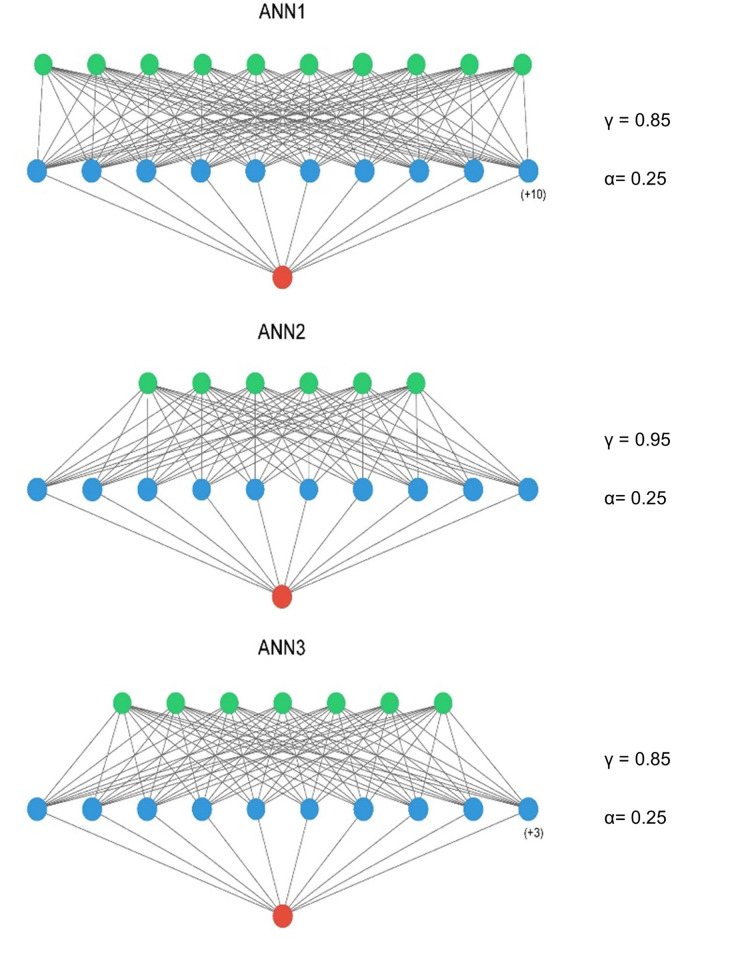
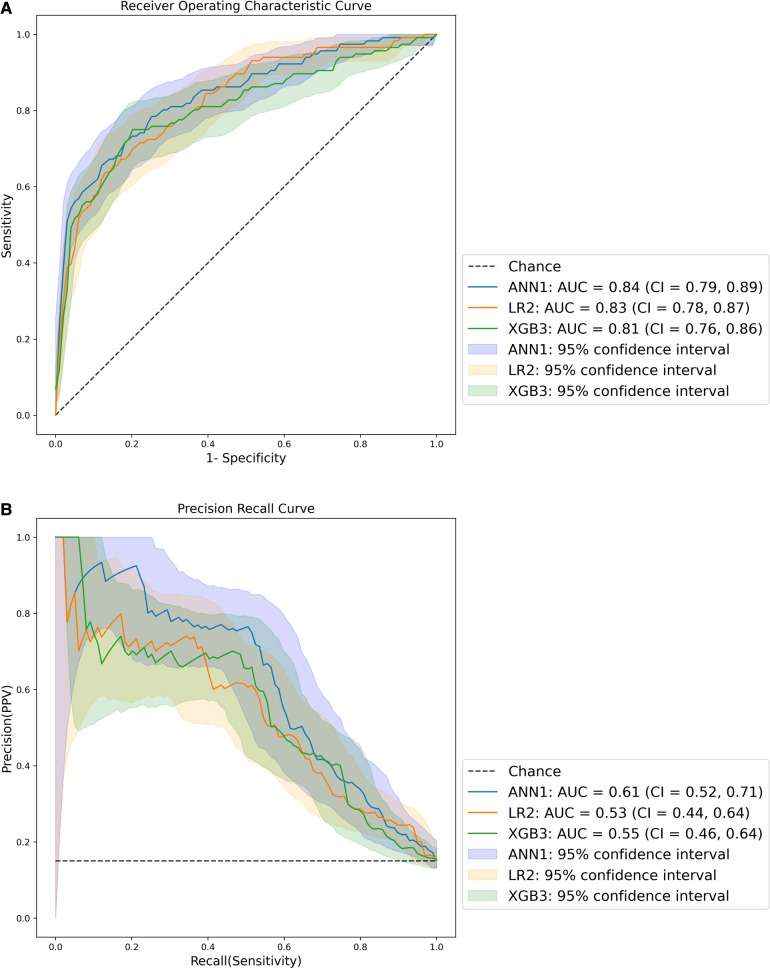
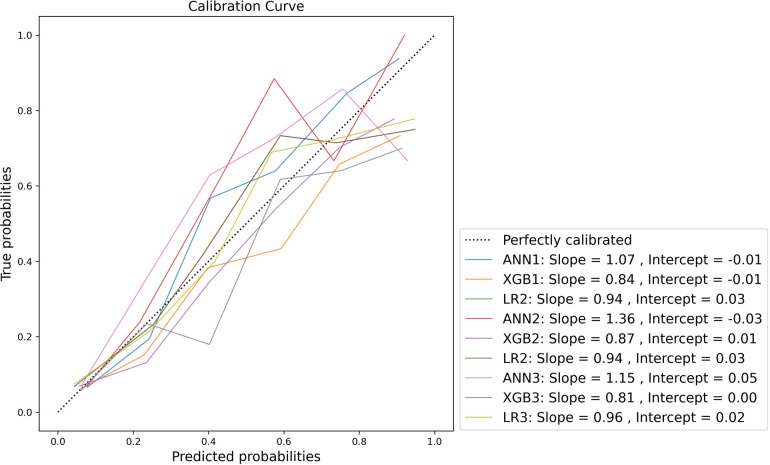
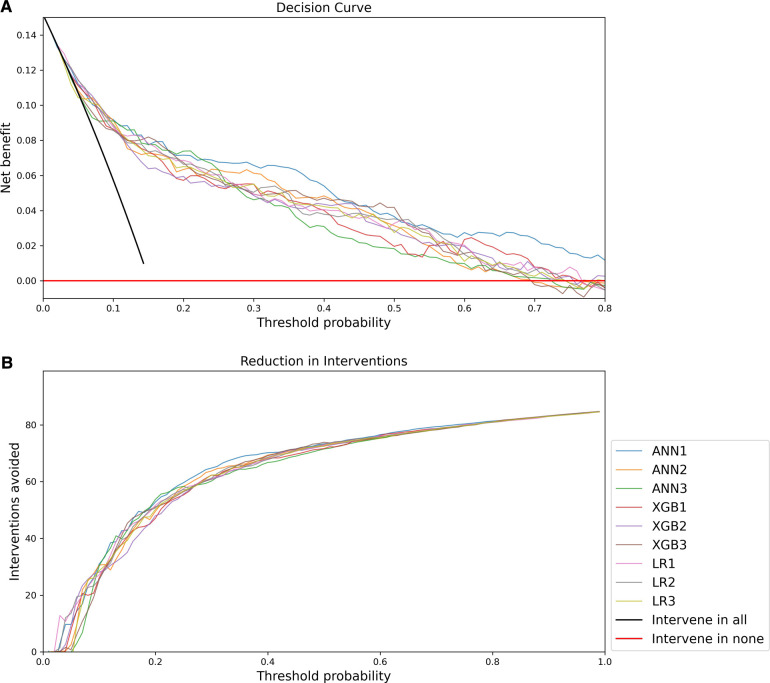
Measurements and main results: 765 patients were included in the data set with 116 instances (15.2%) of the study outcome. Models were developed on three sets of features. Two derived from sequential floating feature selection (one inclusive, one parsimonious) and one from the Akaike information criterion to yield 9 models. All developed models demonstrated good discrimination on cross-validation with mean ROC AUCs greater than 0.8 and mean PRC AUCs greater than 0.53. ANN1, developed on the inclusive feature-et demonstrated the best discrimination with a ROC AUC of 0.84 and a PRC AUC of 0.64 Model calibration was variable, with most models demonstrating weak calibration. Decision curve analysis demonstrated that all models were superior to baseline strategies, with ANN1 demonstrating the highest net benefit.
Conclusions: All models demonstrated satisfactory performance, with the best performing model in cross-validation being an ANN model. Given the good performance of less complex models, however, these models should also be considered, given their advantage in ease of implementation in practice. An internal validation study is now being conducted to further assess performance with a view to external validation.
Keywords: children; critical care; machine learning; neural networks; severity of illness; triage.
© 2022 Pienaar, Sempa, Luwes, George and Brown.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Elicitation of domain knowledge for a machine learning model for paediatric critical illness in South Africa.Front Pediatr. 2023 Feb 21;11:1005579. doi: 10.3389/fped.2023.1005579. eCollection 2023. Front Pediatr. 2023. PMID: 36896402 Free PMC article.
-
A validation of machine learning models for the identification of critically ill children presenting to the paediatric emergency room of a tertiary hospital in South Africa: A proof of concept.South Afr J Crit Care. 2024 Nov 25;40(3):e1398. doi: 10.7196/SAJCC.2024.v40i3.1398. eCollection 2024. South Afr J Crit Care. 2024. PMID: 39911207 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
An Artificial Neural Network Model for Pediatric Mortality Prediction in Two Tertiary Pediatric Intensive Care Units in South Africa. A Development Study.Front Pediatr. 2022 Feb 25;10:797080. doi: 10.3389/fped.2022.797080. eCollection 2022. Front Pediatr. 2022. PMID: 35281234 Free PMC article.
-
[Construction of a predictive model for in-hospital mortality of sepsis patients in intensive care unit based on machine learning].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Jul;35(7):696-701. doi: 10.3760/cma.j.cn121430-20221219-01104. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37545445 Chinese.
Cited by
-
Elicitation of domain knowledge for a machine learning model for paediatric critical illness in South Africa.Front Pediatr. 2023 Feb 21;11:1005579. doi: 10.3389/fped.2023.1005579. eCollection 2023. Front Pediatr. 2023. PMID: 36896402 Free PMC article.
-
A validation of machine learning models for the identification of critically ill children presenting to the paediatric emergency room of a tertiary hospital in South Africa: A proof of concept.South Afr J Crit Care. 2024 Nov 25;40(3):e1398. doi: 10.7196/SAJCC.2024.v40i3.1398. eCollection 2024. South Afr J Crit Care. 2024. PMID: 39911207 Free PMC article.
-
Use of artificial intelligence in healthcare in South Africa: A scoping review.Health SA. 2025 Jul 14;30:2977. doi: 10.4102/hsag.v30i0.2977. eCollection 2025. Health SA. 2025. PMID: 40800148 Free PMC article. Review.
References
-
- Hodkinson P, Argent A, Wallis L, Reid S, Perera R, Harrison S, et al. Pathways to care for critically ill or injured children: a cohort study from first presentation to healthcare services through to admission to intensive care or death. PLoS One. (2016) 11(1):1–17. 10.1371/journal.pone.0145473 - DOI - PMC - PubMed
-
- Patel M, Maconochie I. Triage in children. Trauma. (2008) 10(4):239–45. 10.1177/1460408608096795 - DOI
-
- South African Triage Group. The South African Triage Scale Training Manual 2012. South African Triage Scale Training Manual 2012. (2012);1–34 p.
Grants and funding
LinkOut - more resources
Full Text Sources