

Image quality and related outcomes of the ShuntScope for catheter implantation in pediatric hydrocephalus-experience of 65 procedures
- PMID: 36459211
- PMCID: PMC10024658
- DOI: 10.1007/s00381-022-05776-1
Image quality and related outcomes of the ShuntScope for catheter implantation in pediatric hydrocephalus-experience of 65 procedures
Abstract
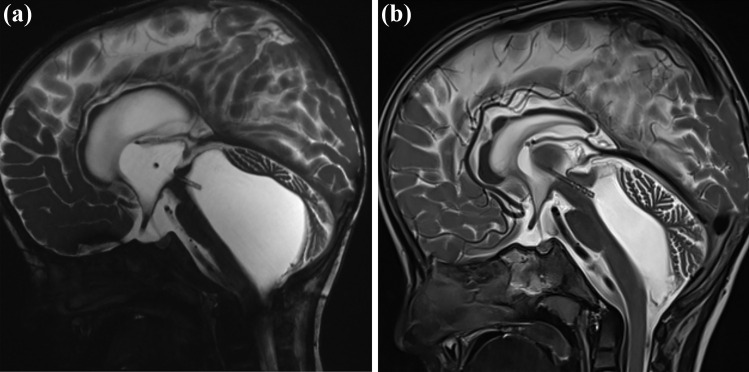
Purpose: Ventricular catheter implantation in pediatric hydrocephalus can become a highly challenging task due to abnormal anatomical configuration or the need for trans-aqueductal stent placement. Transluminal endoscopy with the ShuntScope has been invented to increase the rate of successful catheter placements. This study aims to evaluate ShuntScope's image qualities and related surgical outcomes in the pediatric population.
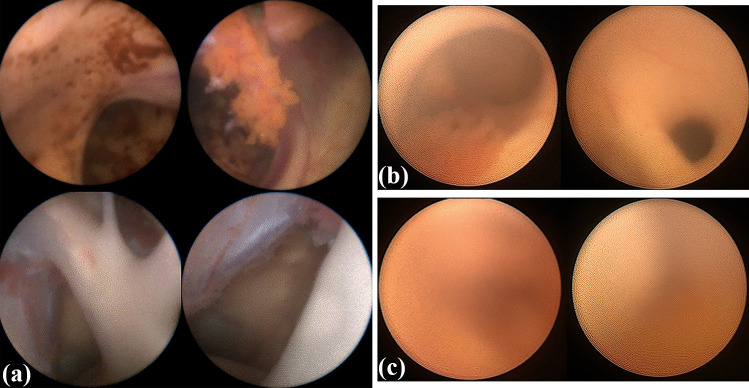
Methods: A retrospective analysis of all pediatric patients undergoing ventricular catheter placement using the ShuntScope from 01/2012 to 01/2022 in the author's department was performed. Demographic, clinical, and radiological data were evaluated. The visualization quality of the intraoperative endoscopy was stratified into the categories of excellent, medium, and poor and compared to the postoperative catheter tip placement. Follow-up evaluation included the surgical revision rate due to proximal catheter occlusion.
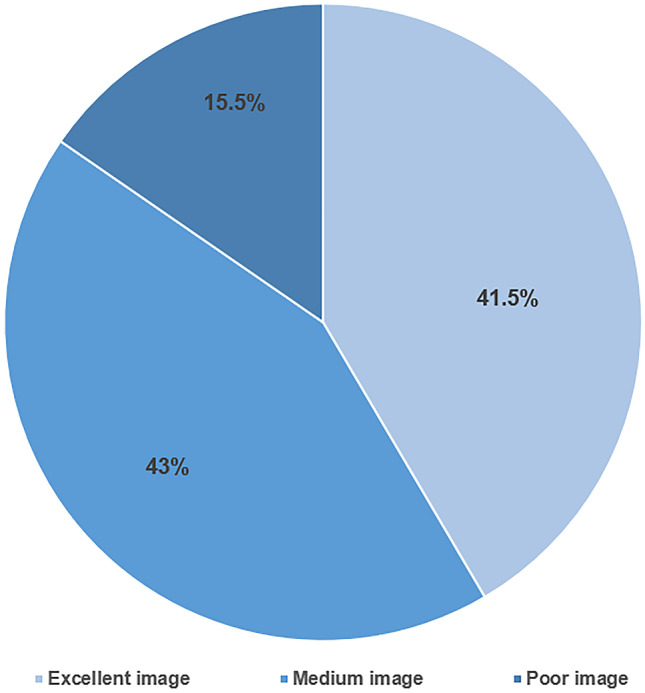
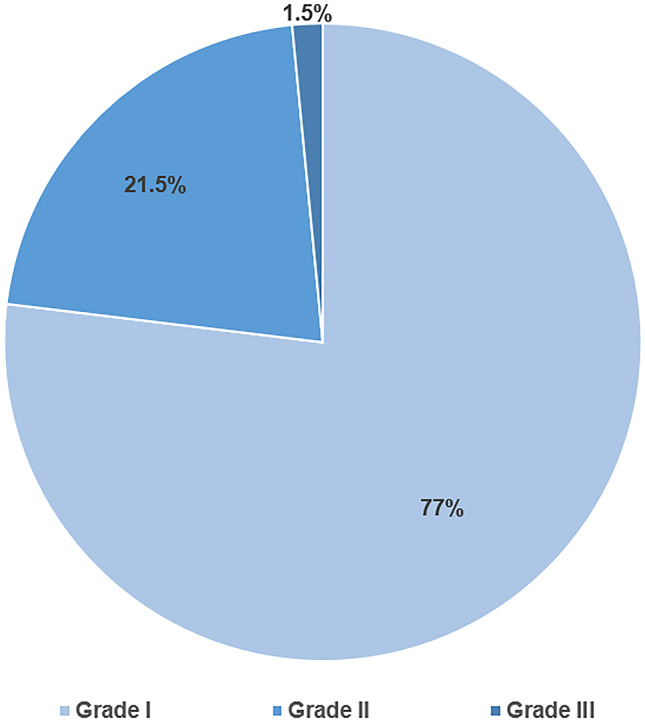
Results: A total of 65 ShuntScope-assisted surgeries have been performed on 51 children. The mean age was 5.1 years. The most common underlying pathology was a tumor- or cyst-related hydrocephalus in 51%. Achieved image quality was excellent in 41.5%, medium in 43%, and poor in 15.5%. Ideal catheter placement was achieved in 77%. There were no intraoperative complications and no technique-related morbidity associated with the ShuntScope. The revision rate due to proximal occlusion was 4.61% during a mean follow-up period of 39.7 years. No statistical correlation between image grade and accuracy of catheter position was observed (p-value was 0.290).
Conclusion: The ShuntScope can be considered a valuable addition to standard surgical tools in treating pediatric hydrocephalus. Even suboptimal visualization contributes to high rates of correct catheter placement and, thereby, to a favorable clinical outcome.
Keywords: Endoscopy; Pediatric hydrocephalus; ShuntScope; Shunting; Ventricular catheter.
© 2022. The Author(s).
Conflict of interest statement
There are no competing financial or non-financial interests. Joachim Oertel acted as a consultant for Karl Storz Company for spine surgery until 2020. No conflicting interests exist for the material and technique mentioned in the publication.
Figures





References
-
- Hsia CC, Chen YH, Wu HY, Liu MY. The misplacement of the external ventricular drain by the freehand method in emergent neurosurgery. Acta Neurol Belg. 2011;111:22–28. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
