

Effectiveness of mHealth Interventions in the Control of Lifestyle and Cardiovascular Risk Factors in Patients After a Coronary Event: Systematic Review and Meta-analysis
- PMID: 36459396
- PMCID: PMC9758644
- DOI: 10.2196/39593
Effectiveness of mHealth Interventions in the Control of Lifestyle and Cardiovascular Risk Factors in Patients After a Coronary Event: Systematic Review and Meta-analysis
Abstract
Background: Coronary artery disease is the main cause of death and loss of disability-adjusted life years worldwide. Information and communication technology has become an important part of health care systems, including the innovative cardiac rehabilitation services through mobile phone and mobile health (mHealth) interventions.
Objective: In this study, we aimed to determine the effectiveness of different kinds of mHealth programs in changing lifestyle behavior, promoting adherence to treatment, and controlling modifiable cardiovascular risk factors and psychosocial outcomes in patients who have experienced a coronary event.
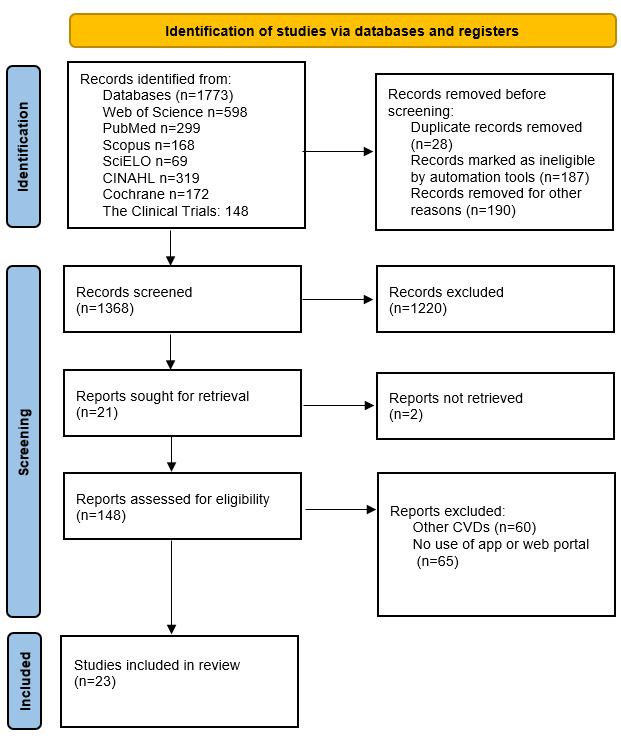
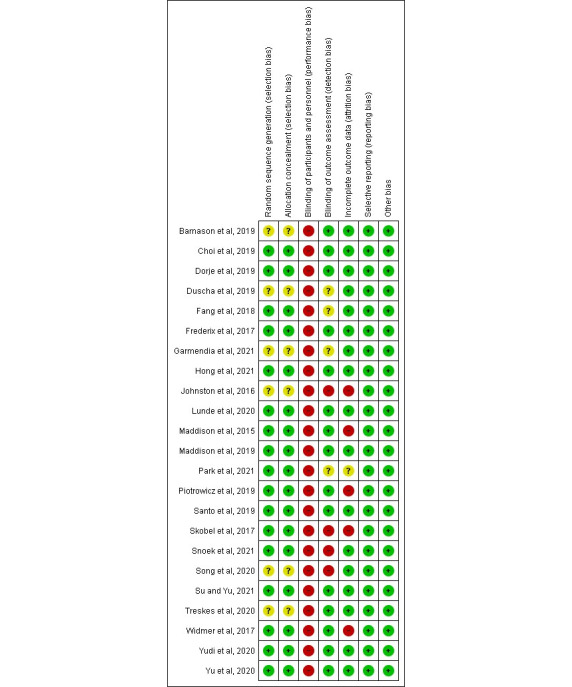
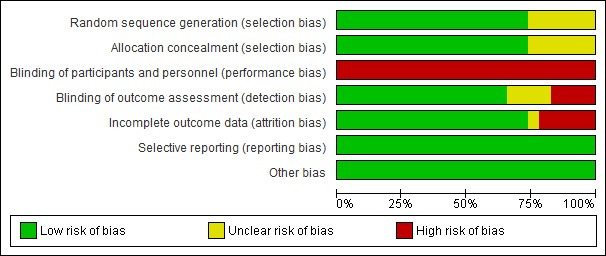
Methods: A systematic review of the literature was performed following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A thorough search of the following biomedical databases was conducted: PubMed, Embase, Web of Science, SciELO, CINAHL, Scopus, The Clinical Trial, and Cochrane. Articles that were randomized clinical trials that involved an intervention consisting of an mHealth program using a mobile app in patients after a coronary event were included. The articles analyzed some of the following variables as outcome variables: changes in lifestyle behavior, cardiovascular risk factors, and anthropometric and psychosocial variables. A meta-analysis of the variables studied was performed with the Cochrane tool. The risk of bias was assessed using the Cochrane Collaboration tool; the quality of the evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation tool; and heterogeneity was measured using the I2 test.
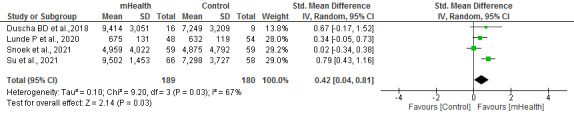
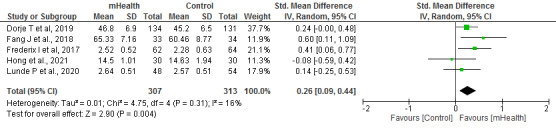
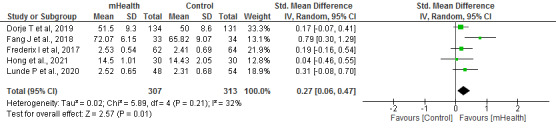
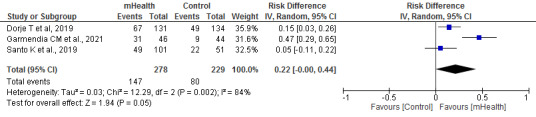
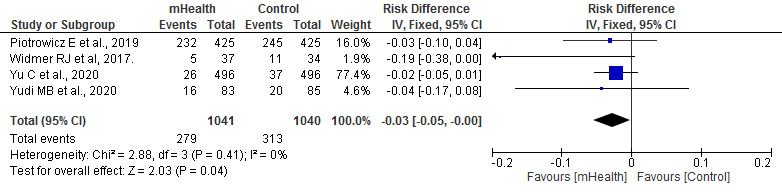
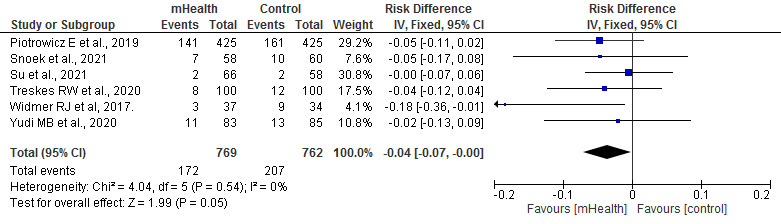
Results: A total of 23 articles were included in the review, and 20 (87%) were included in the meta-analysis, with a total sample size of 4535 patients. Exercise capacity measured using the 6-minute walk test (mean difference=21.64, 95% CI 12.72-30.55; P<.001), physical activity (standardized mean difference [SMD]=0.42, 95% CI 0.04-0.81; P=.03), and adherence to treatment (risk difference=0.19, 95% CI 0.11-0.28; P<.001) were significantly superior in the mHealth group. Furthermore, both the physical and mental dimensions of quality of life were better in the mHealth group (SMD=0.26, 95% CI 0.09-0.44; P=.004 and SMD=0.27, 95% CI 0.06-0.47; P=.01, respectively). In addition, hospital readmissions for all causes and cardiovascular causes were statistically higher in the control group than in the mHealth group (SMD=-0.03, 95% CI -0.05 to -0.00; P=.04 vs SMD=-0.04, 95% CI -0.07 to -0.00; P=.05).
Conclusions: mHealth technology has a positive effect on patients who have experienced a coronary event in terms of their exercise capacity, physical activity, adherence to medication, and physical and mental quality of life, as well as readmissions for all causes and cardiovascular causes.
Trial registration: PROSPERO (International Prospective Register of Systematic Reviews) CRD42022299931; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=299931.
Keywords: acute coronary syndrome; coronary disease; mobile apps; mobile health; mobile phone; smartphone.
©Celia Cruz-Cobo, María Ángeles Bernal-Jiménez, Rafael Vázquez-García, María José Santi-Cano. Originally published in JMIR mHealth and uHealth (https://mhealth.jmir.org), 02.12.2022.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

References
-
- Cardiovascular diseases. World Health Organization. [2021-07-06]. https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 .
-
- Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, Hystad P, Brauer M, Kutty VR, Gupta R, Wielgosz A, AlHabib KF, Dans A, Lopez-Jaramillo P, Avezum A, Lanas F, Oguz A, Kruger IM, Diaz R, Yusoff K, Mony P, Chifamba J, Yeates K, Kelishadi R, Yusufali A, Khatib R, Rahman O, Zatonska K, Iqbal R, Wei L, Bo H, Rosengren A, Kaur M, Mohan V, Lear SA, Teo KK, Leong D, O'Donnell M, McKee M, Dagenais G. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020 Mar;395(10226):795–808. doi: 10.1016/s0140-6736(19)32008-2. - DOI - PMC - PubMed
-
- Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob Health. 2021 Jun;11(2):169–77. doi: 10.2991/jegh.k.201217.001. https://europepmc.org/abstract/MED/33605111 jegh.k.201217.001 - DOI - PMC - PubMed
-
- Nowbar AN, Howard JP, Finegold JA, Asaria P, Francis DP. 2014 global geographic analysis of mortality from ischaemic heart disease by country, age and income: statistics from World Health Organisation and United Nations. Int J Cardiol. 2014 Jun 15;174(2):293–8. doi: 10.1016/j.ijcard.2014.04.096. https://linkinghub.elsevier.com/retrieve/pii/S0167-5273(14)00755-4 S0167-5273(14)00755-4 - DOI - PMC - PubMed
