

Spatially Resolved Single-Cell Assessment of Pancreatic Cancer Expression Subtypes Reveals Co-expressor Phenotypes and Extensive Intratumoral Heterogeneity
- PMID: 36459568
- PMCID: PMC10548885
- DOI: 10.1158/0008-5472.CAN-22-3050
Spatially Resolved Single-Cell Assessment of Pancreatic Cancer Expression Subtypes Reveals Co-expressor Phenotypes and Extensive Intratumoral Heterogeneity
Abstract
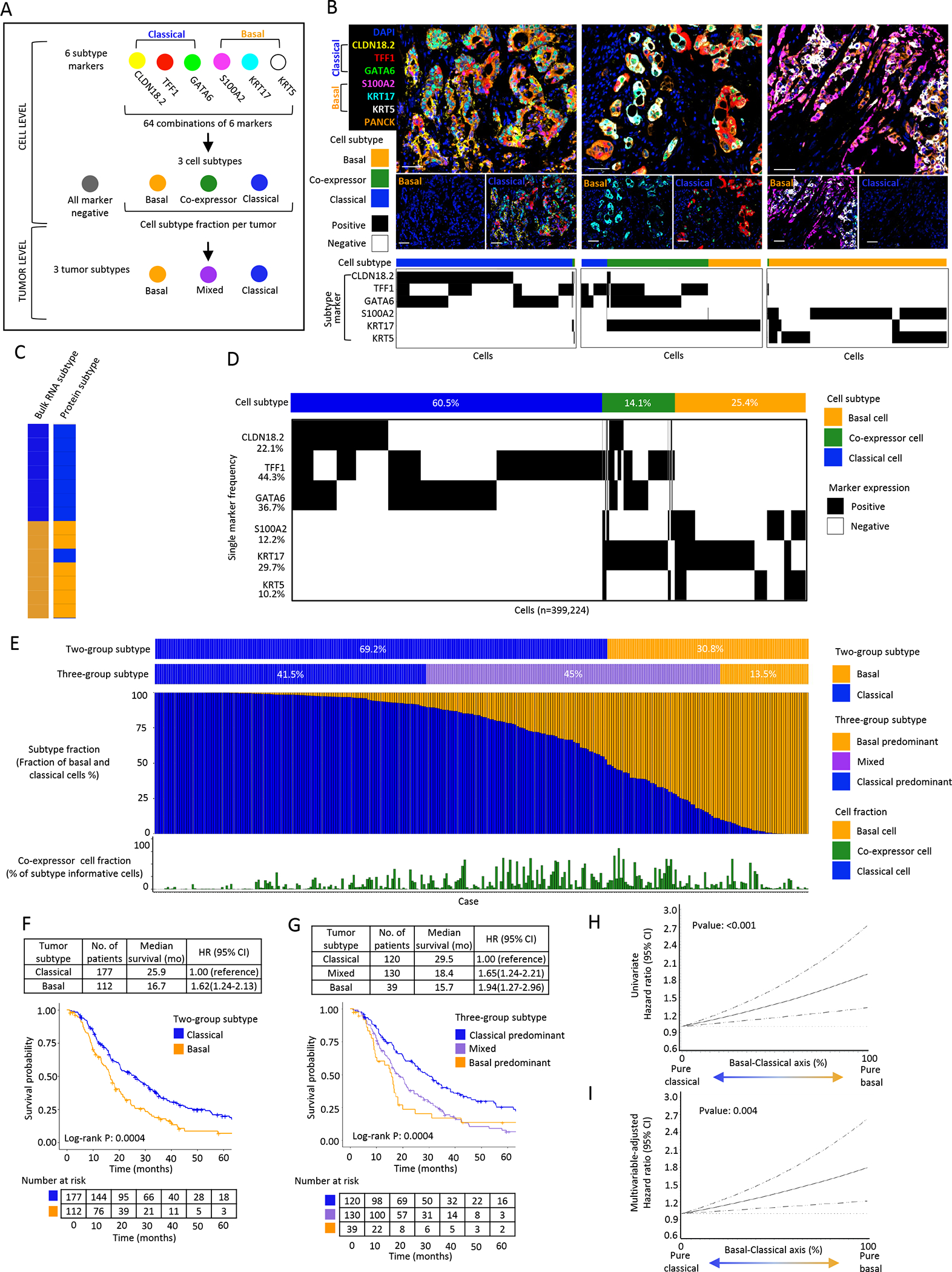
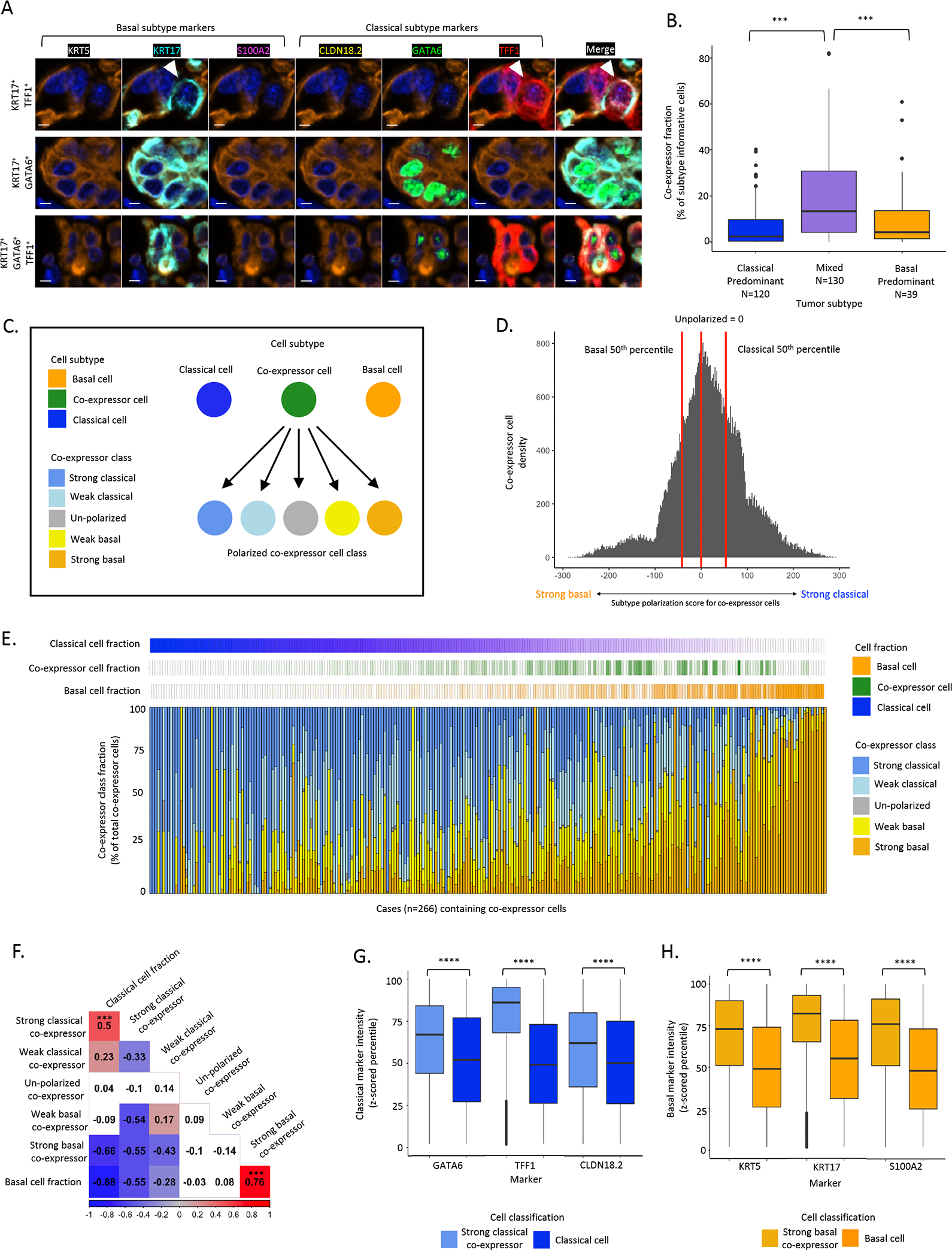
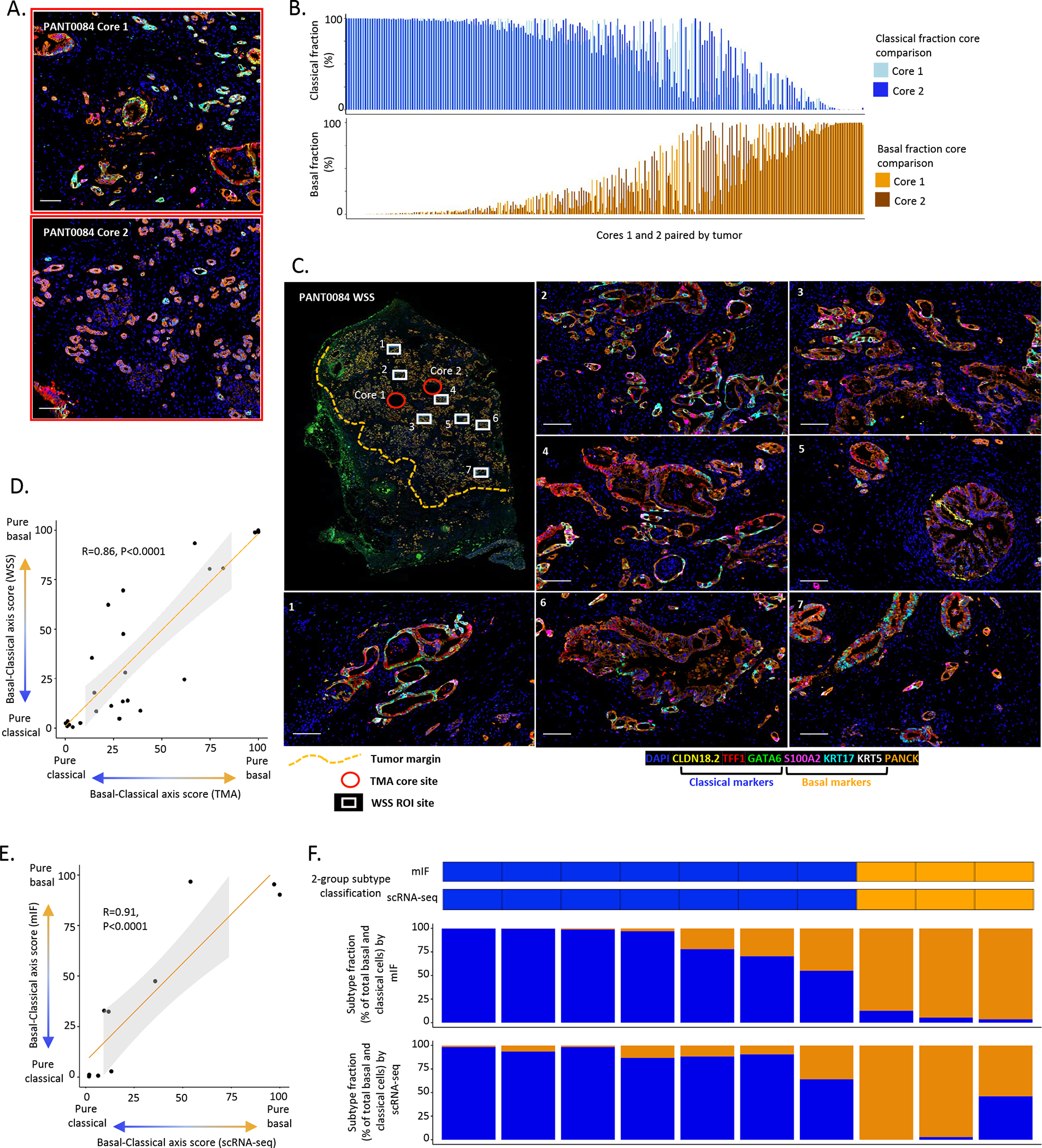
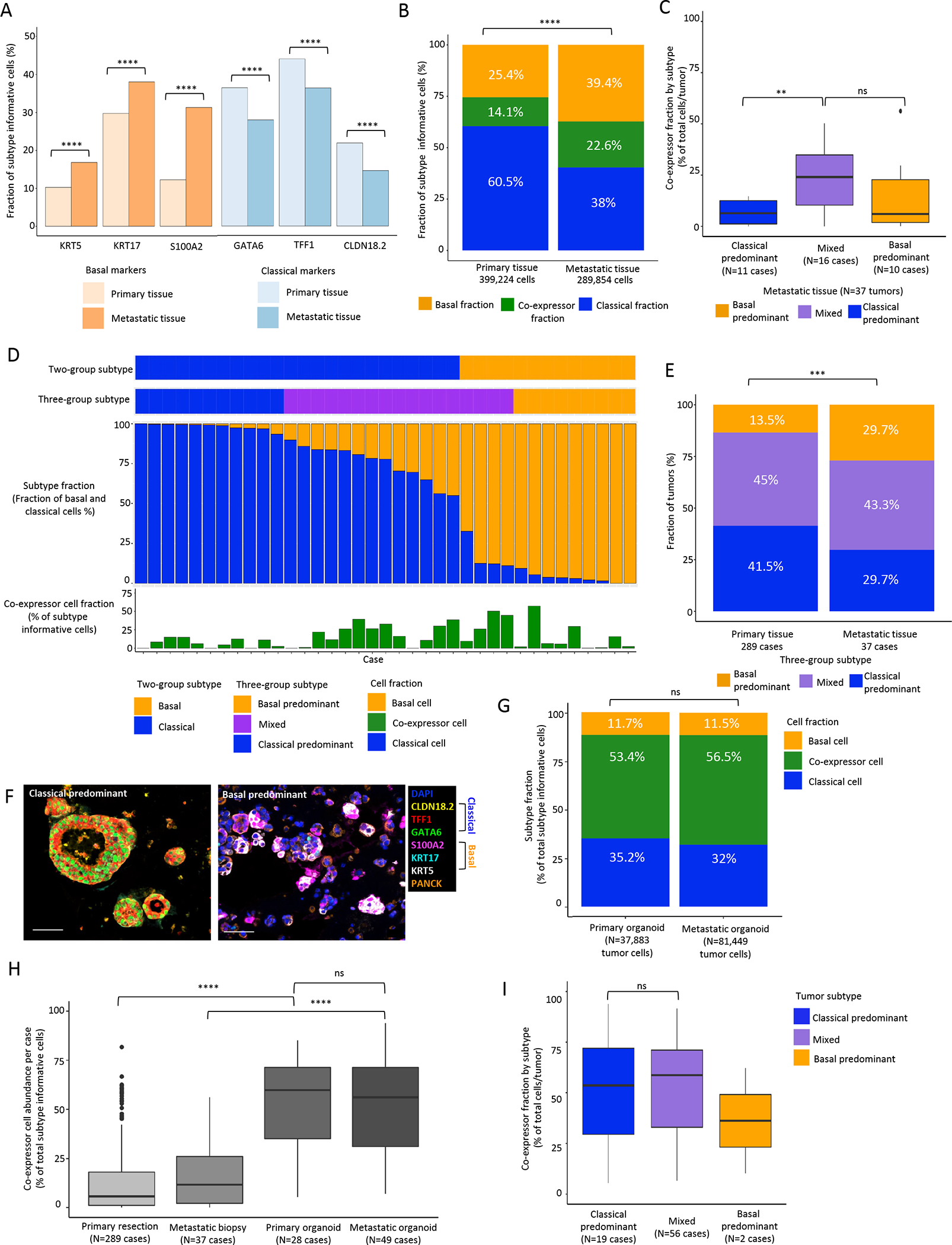
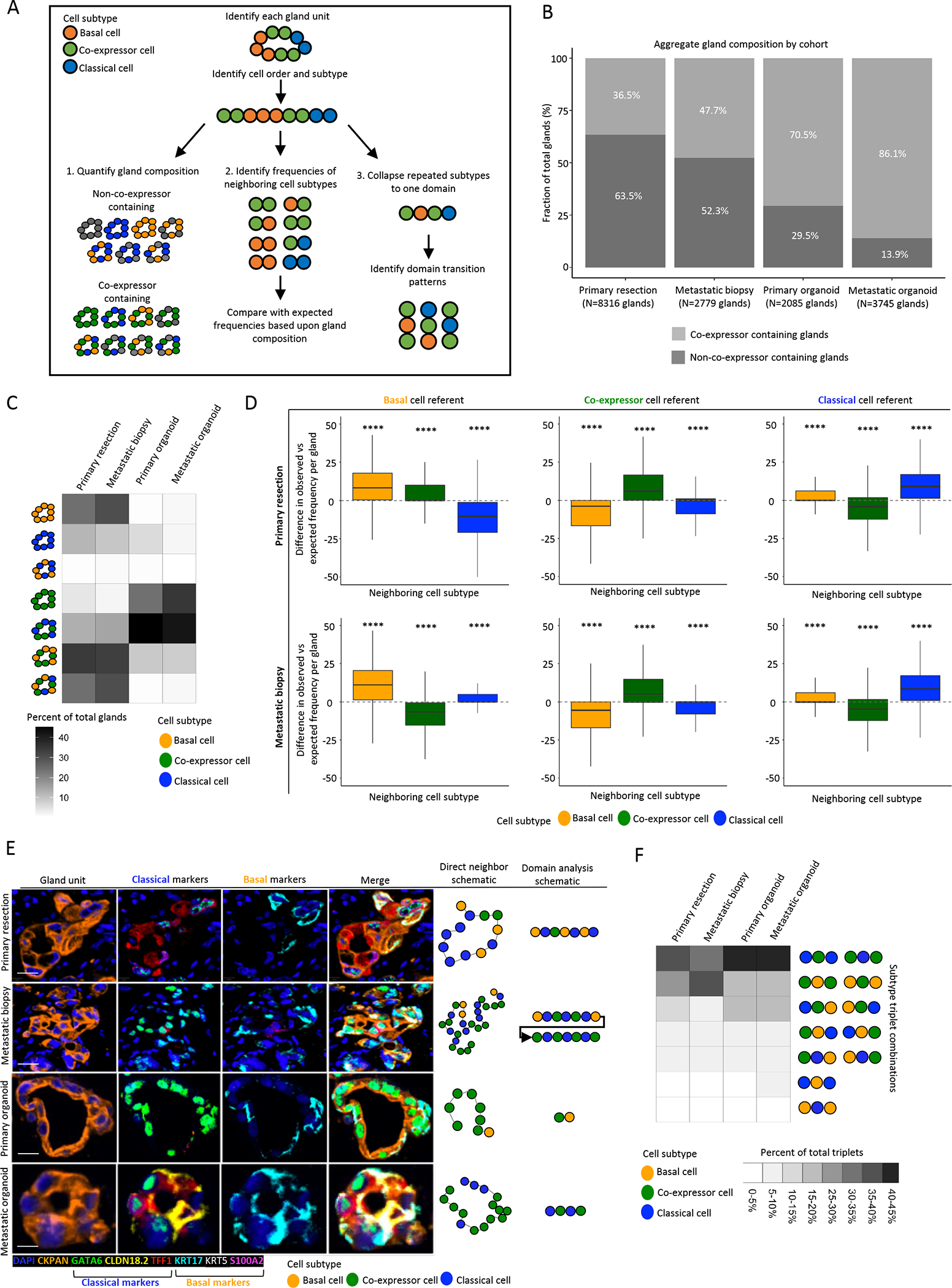
Pancreatic ductal adenocarcinoma (PDAC) has been classified into classical and basal-like transcriptional subtypes by bulk RNA measurements. However, recent work has uncovered greater complexity to transcriptional subtypes than was initially appreciated using bulk RNA expression profiling. To provide a deeper understanding of PDAC subtypes, we developed a multiplex immunofluorescence (mIF) pipeline that quantifies protein expression of six PDAC subtype markers (CLDN18.2, TFF1, GATA6, KRT17, KRT5, and S100A2) and permits spatially resolved, single-cell interrogation of pancreatic tumors from resection specimens and core needle biopsies. Both primary and metastatic tumors displayed striking intratumoral subtype heterogeneity that was associated with patient outcomes, existed at the scale of individual glands, and was significantly reduced in patient-derived organoid cultures. Tumor cells co-expressing classical and basal markers were present in > 90% of tumors, existed on a basal-classical polarization continuum, and were enriched in tumors containing a greater admixture of basal and classical cell populations. Cell-cell neighbor analyses within tumor glands further suggested that co-expressor cells may represent an intermediate state between expression subtype poles. The extensive intratumoral heterogeneity identified through this clinically applicable mIF pipeline may inform prognosis and treatment selection for patients with PDAC.
Significance: A high-throughput pipeline using multiplex immunofluorescence in pancreatic cancer reveals striking expression subtype intratumoral heterogeneity with implications for therapy selection and identifies co-expressor cells that may serve as intermediates during subtype switching.
©2022 American Association for Cancer Research.
Conflict of interest statement
Conflict of interest:
B.M.W. declares research funding from Celgene, Eli Lilly & Company, Novartis, and Revolution Medicine, and consulting for Celgene, GRAIL, and Mirati. J.A.N. declares research funding from NanoString, Illumina, and Akoya Biosciences. K.P. declares One-time Pancreatic Advisory Board fee for Celgene (5/2019). One-time HCC Advisory Board fee for Eisai (11/2019). One-time Cholangiocarcinoma Advisory Board for Helsinn/QED (5/2021). R.F.D. declares Advisory Board for Exelixis INC. and Helsinn Healthcare. All other authors declare no potential conflicts of interest.
Figures
References
-
- American Cancer Society. 2020 Cancer Estimates [Internet]. 2020. Available from: https://cancerstatisticscenter.cancer.org/module/yg6E0ZLc
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
