

Interrater Reliability of Expert Electroencephalographers Identifying Seizures and Rhythmic and Periodic Patterns in EEGs
- PMID: 36460472
- PMCID: PMC10136018
- DOI: 10.1212/WNL.0000000000201670
Interrater Reliability of Expert Electroencephalographers Identifying Seizures and Rhythmic and Periodic Patterns in EEGs
Abstract
Background and objectives: The validity of brain monitoring using electroencephalography (EEG), particularly to guide care in patients with acute or critical illness, requires that experts can reliably identify seizures and other potentially harmful rhythmic and periodic brain activity, collectively referred to as "ictal-interictal-injury continuum" (IIIC). Previous interrater reliability (IRR) studies are limited by small samples and selection bias. This study was conducted to assess the reliability of experts in identifying IIIC.
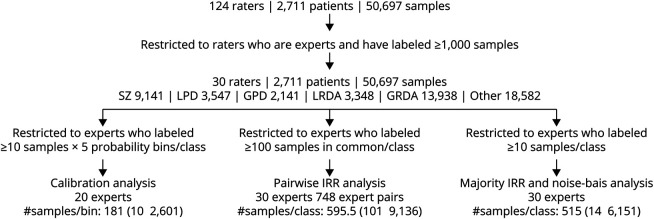
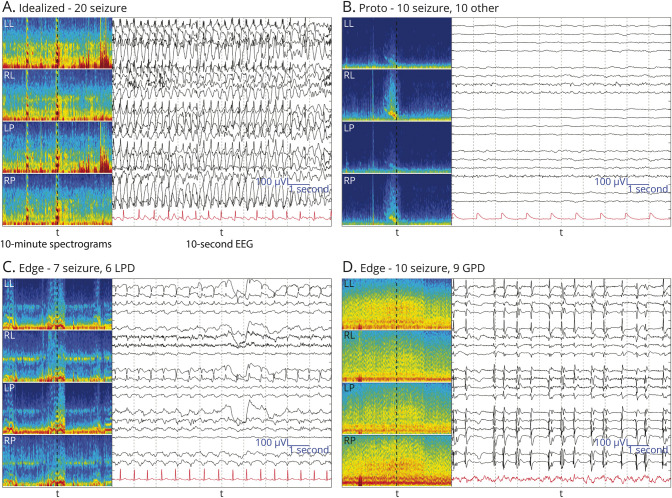
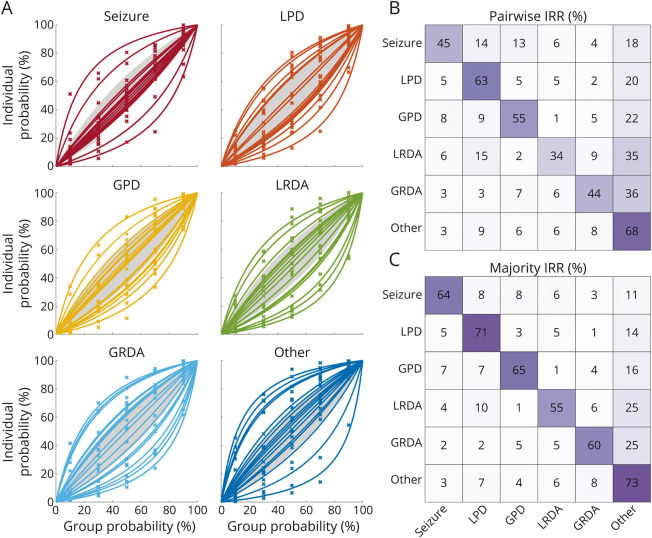
Methods: This prospective analysis included 30 experts with subspecialty clinical neurophysiology training from 18 institutions. Experts independently scored varying numbers of ten-second EEG segments as "seizure (SZ)," "lateralized periodic discharges (LPDs)," "generalized periodic discharges (GPDs)," "lateralized rhythmic delta activity (LRDA)," "generalized rhythmic delta activity (GRDA)," or "other." EEGs were performed for clinical indications at Massachusetts General Hospital between 2006 and 2020. Primary outcome measures were pairwise IRR (average percent agreement [PA] between pairs of experts) and majority IRR (average PA with group consensus) for each class and beyond chance agreement (κ). Secondary outcomes were calibration of expert scoring to group consensus, and latent trait analysis to investigate contributions of bias and noise to scoring variability.
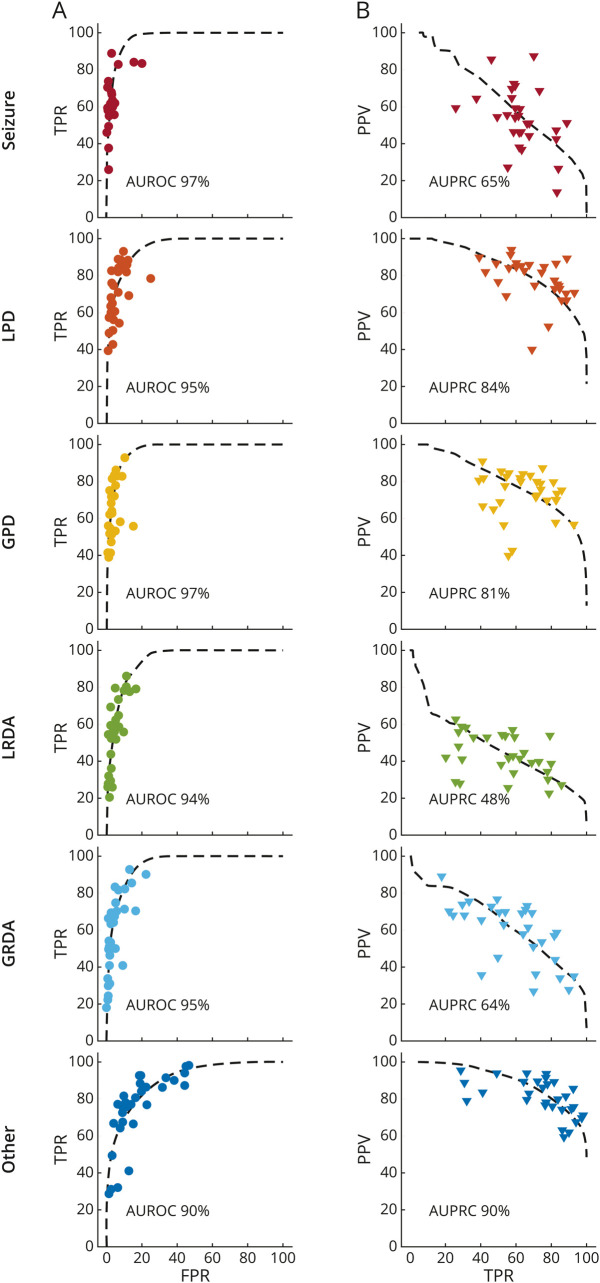
Results: Among 2,711 EEGs, 49% were from women, and the median (IQR) age was 55 (41) years. In total, experts scored 50,697 EEG segments; the median [range] number scored by each expert was 6,287.5 [1,002, 45,267]. Overall pairwise IRR was moderate (PA 52%, κ 42%), and majority IRR was substantial (PA 65%, κ 61%). Noise-bias analysis demonstrated that a single underlying receiver operating curve can account for most variation in experts' false-positive vs true-positive characteristics (median [range] of variance explained ([Formula: see text]): 95 [93, 98]%) and for most variation in experts' precision vs sensitivity characteristics ([Formula: see text]: 75 [59, 89]%). Thus, variation between experts is mostly attributable not to differences in expertise but rather to variation in decision thresholds.
Discussion: Our results provide precise estimates of expert reliability from a large and diverse sample and a parsimonious theory to explain the origin of disagreements between experts. The results also establish a standard for how well an automated IIIC classifier must perform to match experts.
Classification of evidence: This study provides Class II evidence that an independent expert review reliably identifies ictal-interictal injury continuum patterns on EEG compared with expert consensus.
© 2022 American Academy of Neurology.
Conflict of interest statement
The authors report no disclosures relevant to the manuscript. Go to
Figures
Comment in
-
Putting the "Big" in Big Data: Learning to Be Just as (Un)certain as a Clinician at EEG.Neurology. 2023 Apr 25;100(17):799-800. doi: 10.1212/WNL.0000000000207224. Epub 2023 Mar 6. Neurology. 2023. PMID: 36878700 No abstract available.
References
Publication types
MeSH terms
Grants and funding
- R01 NS102190/NS/NINDS NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- RF1 NS120947/NS/NINDS NIH HHS/United States
- F30 NS060325/NS/NINDS NIH HHS/United States
- P20 GM130447/GM/NIGMS NIH HHS/United States
- R01 NS102574/NS/NINDS NIH HHS/United States
- R01 AG029289/AG/NIA NIH HHS/United States
- K24 NS088568/NS/NINDS NIH HHS/United States
- R01 NS111022/NS/NINDS NIH HHS/United States
- R01 NS062092/NS/NINDS NIH HHS/United States
- K23 NS110980/NS/NINDS NIH HHS/United States
- K23 NS112596/NS/NINDS NIH HHS/United States
- R21 NS128641/NS/NINDS NIH HHS/United States
- R01 HL161253/HL/NHLBI NIH HHS/United States
- RF1 AG064312/AG/NIA NIH HHS/United States
- R01 NS126282/NS/NINDS NIH HHS/United States
- R01 NS107291/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials