

Crisaborole efficacy in murine models of skin inflammation and Staphylococcus aureus infection
- PMID: 36461082
- PMCID: PMC10066830
- DOI: 10.1111/exd.14722
Crisaborole efficacy in murine models of skin inflammation and Staphylococcus aureus infection
Abstract
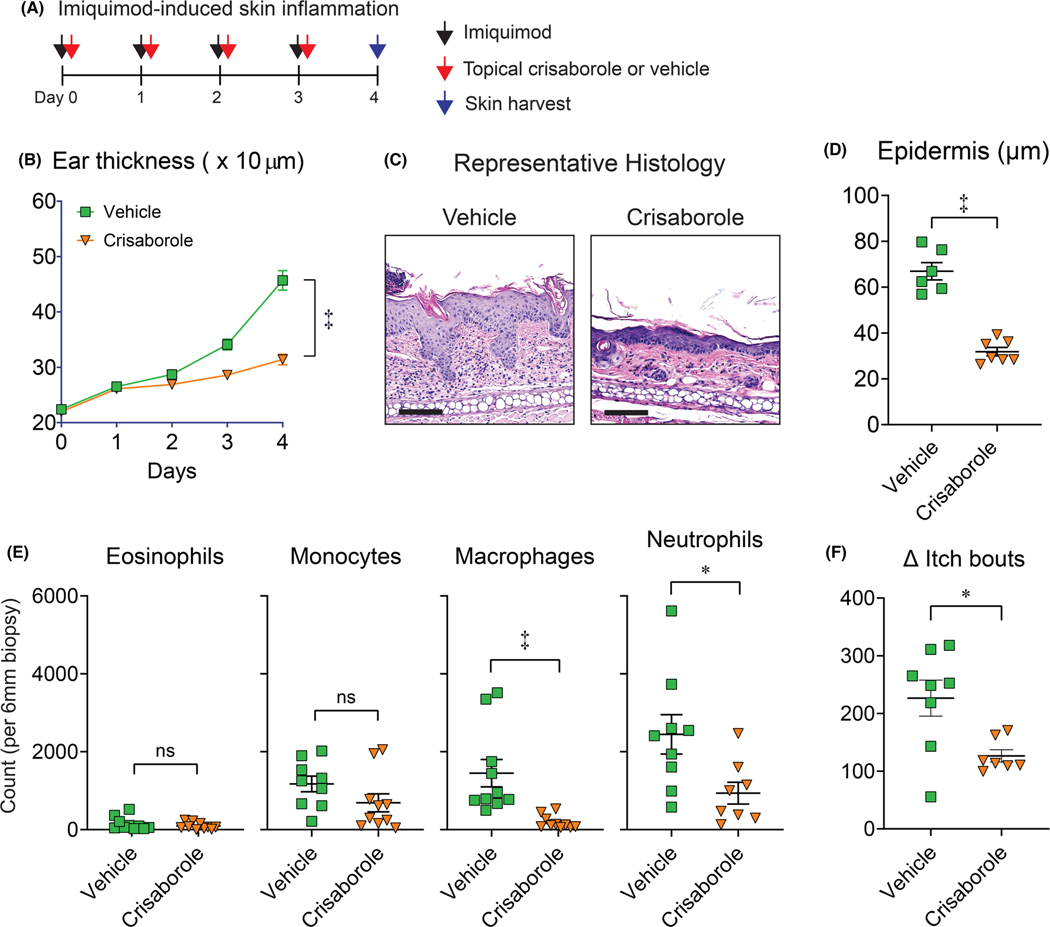
Phosphodiesterase 4 (PDE4) is highly expressed in keratinocytes and immune cells and promotes pro-inflammatory responses upon activation. The activity of PDE4 has been attributed to various inflammatory conditions, leading to the development and approval of PDE4 inhibitors as host-directed therapeutics in humans. For example, the topical PDE4 inhibitor, crisaborole, is approved for the treatment of mild-to-moderate atopic dermatitis and has shown efficacy in patients with psoriasis. However, the role of crisaborole in regulating the immunopathogenesis of inflammatory skin diseases and infection is not entirely known. Therefore, we evaluated the effects of crisaborole in multiple mouse models, including psoriasis-like dermatitis, AD-like skin inflammation with and without filaggrin mutations, and Staphylococcus aureus skin infection. We discovered that crisaborole dampens myeloid cells and itch in the skin during psoriasis-like dermatitis. Furthermore, crisaborole was effective in reducing skin inflammation in the context of filaggrin deficiency. Importantly, crisaborole reduced S. aureus skin colonization during AD-like skin inflammation. However, crisaborole was not efficacious in treating S. aureus skin infections, even as adjunctive therapy to antibiotics. Taken together, we found that crisaborole reduced itch during psoriasis-like dermatitis and decreased S. aureus skin colonization upon AD-like skin inflammation, which act as additional mechanisms by which crisaborole dampens the immunopathogenesis in mouse models of inflammatory skin diseases. Further examination is warranted to translate these preclinical findings to human disease.
Keywords: Staphylococcus aureus; atopic dermatitis; crisaborole; inflammation; psoriasis.
© 2022 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
CONFLICT OF INTEREST
The remaining authors state no conflict of interest.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
